Introduction
Intraductal Papillary mucinous Neoplasm of the Biliary tract (IPNB) is an intraductal mucin producing tumor that is considered as the precursor of cholangiocarcinoma. Intraductal obstructive growth and massive mucin production leads to upstream and downstream biliary dilatation which is considered the most important radiological feature of IPNB [1].
IPNB accounts for 10-15 % of the overall biliary neoplasms [2]. Biliary IPMN (IPNB) is a relatively rare entity with varying imaging findings based on the subtype, radiologists should be aware of this imaging spectrum. Radiological differentiation of IPNB from intraductal cholangiocarcinoma always not possible, due to overlapping features.
Case 1
65-year-old female presented to emergency department with severe abdominal pain, radiating to back of one day duration. There was no history of itching, fever or vomiting, loss of appetite or loss of weight or similar episodes in the past. Clinical examination showed stable vitals, icterus and severe epigastric tenderness. Investigations showed abnormal and elevated liver enzymes (Total Bilirubin: 8.2 mg/dl, Direct Bilirubin: 6 mg/dl, SGOT: 168 IU/L, SGPT: 214 IU/L, ALP: 800 IU/L, Albumin: 2 g/dl, TC: 14.5 k/uL, ESR: 32).
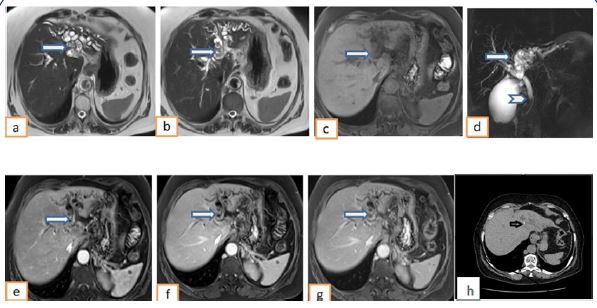
USG showed bilobar intrahepatic biliary radical dilatation (left >right) and dilated CBD, with intraductal isoechoic and echogenic contents. Liver showed mild coarse echotexture, with left lobe atrophy. Gall bladder showed cholelithiasis. MRI with MRCP (Figure 1a-g) showed atrophy of left lobe of liver, with bilobar IHBRD (Left > right), and crowding of intra-biliary ducts. T2 iso to hypointense mildly enhancing small soft tissue densities were seen filling and distending the left sided biliary radicles, up to the confluence. No evidence of soft tissue in the right sided ducts. CBD dilated (10mm) along its entire course, with isointense soft tissue at the distal CBD adjacent to ampulla (Figure 1d). Plain CT showed bilobar IHBRD with 2-3 tiny scattered calcific specks (Figure 1-h). Hence the possibility of biliary IPMN was made with intraductal cholangiocarcinoma as differential.
Spyglass cholangioscopy was done which confirmed mucinous contents. HPE from the tissue hence retrieved showed detached excessively infarcted and necrotic fragment of papillary neoplasm with low grade dysplasia suggesting possibility of biliary IPMN.
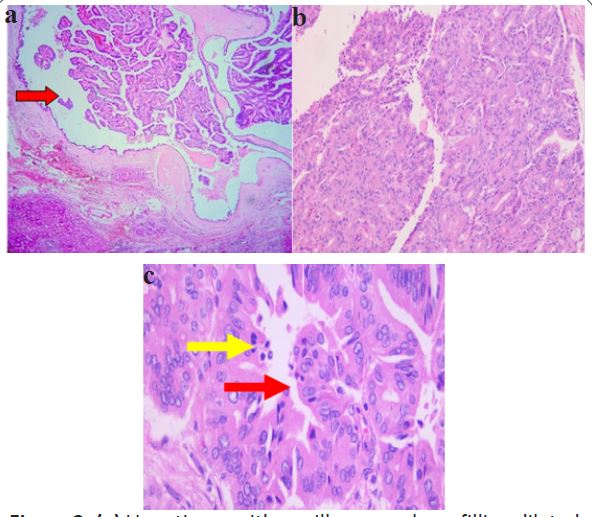
Patient underwent left hepatectomy, CBD excision and Roux-en-Y hepaticojejunostomy. Left hepatectomy specimen showed intraluminal grey white friable granular tumor within the dilated hepatic ducts. Microscopy showed dilated biliary ducts with partly ulcerated mucosa from which a neoplasm is arising with slender to complex papillae predominantly covered by biliary type epithelium and at places with intestinal epithelium. Closely arranged tubular formations and cribriform structures are seen with intraluminal mucinous areas. No invasive component was identified (Figure 2a-c). The final diagnosis given was intraductal papillary neoplasm with high grade intraepithelial neoplasia, biliary type involving the left hepatic duct.
Case 2
55-year-old male presented with backpain along with vague epigastric discomfort for 1 month. No history of loss of appetite, loss of weight, abdominal pain, vomiting, bowel symptoms, pruritus or pale stool. Physical examination was unremarkable. Blood routine showed altered liver enzymes, with predominant elevation of alkaline phosphatase (Total bilirubin: 6.4 mg/dl, Direct bilirubin: 4.8 mg/dl, SGPT: 140 IU/L, SGOT: 180 IU/L, ALP: 600 IU/L, Albumin: 3 g/dl, Total count: 11200/uL, ESR: 24).
USG abdomen showed bilobed cystic lesion in the left lobe of liver, segment II and III, with echogenic solid components along the walls. Left lobar IHBRD was noted distal to the above-mentioned lesion.
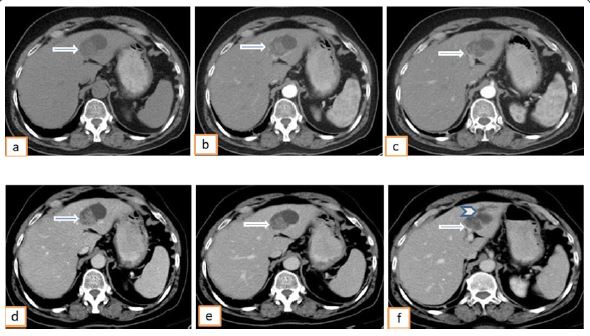
Subsequent contrast enhanced CT abdomen (Figure 3) showed left lobar intrahepatic biliary dilatation involving segment II and III, with a lobulated cystic lesion along the course of the duct. Enhancing polypoidal solid intraductal components noted along the walls of the cystic lesion, with no evidence of involvement of adjacent hepatic parenchyma. Mildly dilated left intrahepatic biliary ducts were noted distal to the lesion with possible communication. Rest of the biliary radicles showed normal wall thickness and enhancement. Right lobe of liver appeared normal. CBD was normal. With the imaging findings, the possibility of biliary cystadenocarcinoma was considered.
The patient was posted for laparoscopic assisted left lateral segmentectomy. The operative findings included an intrahepatic lesion of size 4x5 cm in left lateral segment of liver. His postoperative period was uneventful.
Left lateral segmentectomy specimen showed a cystic lesion with a luminal solid grey white tumour. Microscopy showed cystically dilated bile duct with mural nodules composed of fused papillary structures with central fibrovascular cores lined by columnar epithelium of pancreatico - biliary and gastric type displaying, pseudostratified, enlarged pleomorphic vesicular nuclei, prominent nucleoli and moderate eosinophilic cytoplasm. Cyst wall (dilated bile duct) is lined by similar type of epithelium. Multiple foci of tumour invasion seen in surrounding stroma. Hence the histopathological diagnosis of Intraductal papillary biliary neoplasm with high grade dysplasia and multiple foci of cholangiocarcinoma was made (intraductal growth type).
Discussion
Mucinous cystic neoplasia and IPNB (Intraductal papillary neoplasia of bile ducts) are the two types of cystic hepatic neoplasia. Mucinous cystic neoplasia is characterized by unilocular/septated cystic lesions lined by cuboidal / columnar epithelium with ovarian-like stroma and no communication with the biliary tree. IPNB is also mucin producing neoplasia, showing communication with biliary tree and resultant upstream and downstream dilatation of the biliary tree [1].
Pathology
IPNB is now considered as a distinct biliary disease entity proposed by WHO and published in the Classification of Digestive System Tumours 5th edition (2019). Biliary papillomatosis or biliary papilloma are the other WHO accepted terminologies [9]. IPNB accounts for 10-15% of the overall biliary neoplasms [2]. In Asia, IPNB accounts for 9.9-30% of bile duct tumours [3] as compared to the Western countries where the prevalence of IPNB is around 7-11 % of the total biliary neoplasia [3].
Hepatolithiasis, parasitic infestation, primary sclerosing cholangitis, biliary malformation, and polypoid syndromes like FAP and Gardner syndrome are considered as risk factors for IPNB, all of which causes chronic biliary inflammation [3] which in turn induces the production of reactive oxygen species and reactive nitrogen species, resulting in DNA damage, and plays an important role in carcinogenesis [4].
It is believed that IPNB and Pancreatic IPMN have similar genetic and molecular oncologic pathways [5]. Despite the similarities, the association with high grade dysplasia, invasive carcinoma, advanced stage disease and worse prognosis is higher for IPNB as compared with pancreatic IPMN [6]. IPNB is considered to be the precursor of cholangiocarcinoma in addition to biliary intraepithelial neoplasia, hence familiarity with the imaging findings of this pathology is essential for early diagnosis and curative resection. IPNB follows an adenoma carcinoma sequence with multiple genetic mutations and alterations associated with the same. As per the literature 40-80% of patients with IPNB harbours invasive intraductal cholangiocarcinoma at presentation [6]. Our first case, though it showed multifocal IPNB, had no evidence of invasive component. Our second case had purely intrahepatic IPNB with multiple foci of invasion suggestive of multifocal cholangiocarcinoma. However, the prognosis of cholangiocarcinoma associated with IPNB is better as compared to those not associated with IPNB, likely due to indolent nature of IPNB [7]. A higher association of invasive carcinoma in extrahepatic IPNB associated with biliary dilatation, was illustrated by Ogawa et al in his study [8].
Radiology
The median age of presentation of biliary IPMN is 50-60 years with male preponderance. A significant number of patients remain asymptomatic (12%), with incidental detection during evaluation for other symptoms. Rest of them may present with recurrent episodes of abdominal pain, cholangitis and jaundice, as a result of recurrent biliary obstruction from sloughed friable intraductal masses and resultant abnormal LFT [6]. 42% of the patients show abnormal elevation of CA 19-9 levels [6]. The level of CA 19-9 correlates with the tumor burden and degree of invasiveness.
The biliary dilatation, intraductal mass and the complications can be recognised by USG, CT and MRI. Spyglass Cholangioscopy helps in assessment of superficial spread of lesion and to secure tissue for diagnosis. MRCP in the most sensitive modality in diagnosis and characterisation of ductal pathology, followed by CT and USG.
USG is often the first line investigation in patients with obstructive jaundice, which in turn shows isoechoic/hyperechoic lobulated intraductal lesions which is difficult to be distinguished from inspissated sludge and cholangiocarcinoma. Sometimes USG shows dilated intrahepatic biliary radicles with irregular contour of the ducts and no definite mass, likely due to the adherent sessile soft tissue. The preserved bile duct walls reflect the low-grade nature of the disease [10].
An intraductal mass with upstream and downstream dilatation of the biliary radicles is the most common imaging pattern described in the literature. Other imaging appearances includes plaque like mass with stricture, mural nodules and frond like appearances. Disproportionate ductal dilatation due to mucin hypersecretion is also described. Aneurysmal dilatation of biliary ducts is seen in intrahepatic IPNB. However, if there is only biliary dilatation with no visible mass, segment/lobe with the most dilated ducts should be subjected to scrutiny [6].
IPNB predominantly affects the left sided ductal system. Both of our cases also followed this pattern, as mentioned in the literature.
Based on the imaging appearances on cross sectional modalities, IPNB can be classified into 4 types [10] (Figure 4).
Type I: Upstream and downstream aneurysm dilatation of the biliary radicles with fungating polypoidal intraductal mass; upstream dilatation secondary to obstruction caused by the tumor and downstream dilatation due to excess mucin production which obstructs the ampulla
Type II: Intraductal fungating mass without mucin production, with only upstream dilatation of the biliary ducts.
Type III: Multiple intraductal fungating lobulated soft tissue lesions with variable mucin production associated with aneurysmal dilatation of branches of the bile ducts depending on the degree of mucin production.
Type IV: Superficial spreading tumor which could not be detected radiographically. Excessive mucin production with resultant aneurysmal dilatation of the ductal system. This variant is prone to rupture and cause pseudomyxoma peritonei and also result in fistulous communications.
Our case 1 could be classified as type I IPNB, showing intraductal polypoidal mass, with upstream and downstream dilatation of ducts, and mucin production.
Our second case could be possibly type III IPNB, with focal aneurysmal dilatation of the intrahepatic biliary radicle, with upstream IHBRD.
IPNB shows early enhancement in the late arterial phase and no enhancement in the delayed phase due to the lack of fibrous component within the lesion. This is one of the differences between IPNB and intra ductal cholangiocarcinoma, which in turn shows progressive centripetal delayed enhancement due to the fibrotic components [10]. However, this single radiological finding alone cannot differentiate between these two entities.
Complications of IPNB includes invasive cholangiocarcinoma, hepato-gastric/hepato-pancreatic fistula formation and rupture of the mucin distended bile ducts with resultant pseudomyxoma peritonei [10]. There are very few case reports where seedling of needle tract following percutaneous biopsy have been reported.
Recurrent pyogenic icteric type of cholangitis with intraductal calculi, intraductal cholangiocarcinoma, intraductal metastases, hepatocellular carcinoma, Caroli’s disease, mucinous cystadenoma/cystadenocarcinoma are the most common differentials. Type 4 IPNB is difficult to be differentiated from pancreatic/ampullary/periampullary carcinoma if ductal dilatation involves extrahepatic duct up to the ampulla [10].
Surgery is the definitive management of IPNB without metastases/no nodal involvement [10]. If confined to a segment, segmentectomy; if confined to a lobe, lobectomy; if extensive superficial spreading type of IPNB, liver transplantation and pancreaticoduodenectomy may be warranted (again contraindicated in patients with distant metastases and positive lymph nodes). For poor surgical candidates, RFA and Argon Plasma Coagulation (APC) are under trial for treatment of IPNB.
Prognosis is favourable after surgical treatment with 5-year survival rate of approximately 80%. The undetected lesions which are usually remote from the main tumor and margin positive resection (R1) are the major factors responsible for recurrence [10].
Therefore, for better outcome, meticulous preoperative assessment of the extent of the tumor, margin negative resection and regular follow-up of every 3 to 6 months are recommended. There are no definite guidelines regarding the follow up of postoperative cases of IPNB. However, in practice, USG abdomen with LFT and serum Ca 19-9 level monitoring is done in most of the centres once in 3 months for 1-2 years and once in 6 months thereafter.
Conclusion
The probability of IPNB should be kept in mind in cases where there is diffuse upstream and downstream dilatation of the biliary system with intraductal mass, as well as cystic hepatic lesions communicating with bile duct. Also, when there is lobar or segmental bile duct dilatation without a visible mass and with severe hepatic parenchymal atrophy of the affected liver, biliary IPNB should be included in the differential. Early curative surgical resection is the corner stone in management of IPNB given the high risk for malignancy and for recurrent cholangitis and obstructive jaundice in non-malignant cases. IPNB has better survival rates as compared with conventional cholangiocarcinoma, however differentiation of IPNB from cholangiocarcinoma is predominantly based of pathological degree of invasiveness.
Learning points
• IPNB is a massive mucin producing biliary neoplasia, which is considered to be the precursor of cholangiocarcinoma.
• Radiology alone cannot distinguish between IPNB and cholangiocarcinoma; though the enhancement characteristics of these lesions vary, there is often an overlap of imaging findings.
• Aneurysmal dilatation of the biliary radicles is considered to be pathognomonic of IPNB.
• All etiologies which causes chronic biliary inflammation like hepatolithiasis, parasitic infestation, primary sclerosing cholangitis, biliary malformation, and polypoid syndromes like FAP and Gardner syndrome are risk factors for IPNB.
• Biliary IPNB and Pancreatic IPMN have similar genetic and molecular oncologic pathways.
• There are 4 types of IPNB; based on the morphology.
• Differentials include recurrent pyogenic cholangitis, intraductal cholangiocarcinoma, intraductal metastases, Caroli’s disease, mucinous cystadenoma / cystadenocarcinoma and pancreatic / ampullary / peri ampullay carcinoma which causes upstream biliary dilatation.
• Surgery is the cornerstone of treatment.
Informed consent: Written informed consent was obtained from the patient(s) for publication of this case review, including accompanying images.
References
- Atoosa Adibi, Niloufar Shabanikia, Abolfazl Taheri. Intraductal papillary mucinous neoplasm of biliary ducts: Literature review and a case report with emphasis on radiological manifestation. JRMS. 2020; 25: 114.
- Saumya Pandey, Nitin Agarwal, Vidushi Gupta, Ashok Sharma, Anil Aggarwal, Sunita Gupta, et al. Diagnosing rare intraductal biliary neoplasms – Intraductal papillary neoplasm of the bile duct: A case report with typical imaging findings. SA JRadiol. 2022; 26: 2387.
- Hyo Jung Park, So Yeon Kim, Hyoung Jung Kim, Seung Soo Lee, Gil Sun Hong, Jae Ho Byun, et al. Intraductal Papillary Neoplasm of the Bile Duct: Clinical, Imaging, and Pathologic Features. AJR. 2018; 211.
- Aishima S, Kubo Y, Tanaka Y, Oda Y. Histological Features of Precancerous and Early Cancerous Lesions of Biliary Tract Carcinoma. J Hepatobiliary Pancreat Sci. 2014; 21: 448–52.
- Flavio G Rocha, Hwajeong Lee, Nora Katabi, Ronald P DeMatteo, Yuman Fong, Michael I D’Angelica, et al. Intraductal Papillary Neoplasm of the Bile Duct: A Biliary Equivalent to Intraductal Papillary Mucinous Neoplasm of the Pancreas? Hepatology. 2012.
- Mattew H Lee, Venkata S Katabathina, Meghan G Lubnar, Hardik Shah, Srinivasa R Prasad, Kristina A, et al. Mucin producing Cystic hepatobiliary neoplasams: Updated Nomenclature and clinical, pathological and imaging features: Radiographics. 2021.
- Anam Aslam, Ashish P Wasnik, Jiaqui Shi, Vaibhav Sahai, Mishal Lala. Intraductal papillary neoplasm of the bile duct (IPNB): CT and MRI appearance with radiology-pathology Correlation. Clin Imaging. 2020; 66: 10-17
- Ogawa H. CT findings of intraductal papillary neoplasia of bile duct: assessment with multiphase contrast enhanced examination using multi-detector CT. Clin Radiol. 2012; 67: 224-231
- Kubota K, Jang JY, Nakanuma Y, Jang KT, Haruyama Y, Fukushima N, et al. clinicopathological characteristics of intraductal papillary neoplasia of bile duct: A Japan Korea collaborative study. J Hepatobilairy Pancreat Sci. 2020; 27: 581-597.
- David J Ritchie, Kanenori Okamoto, Stacey L. White; Intraductal papillary mucinous neoplasm of the biliary tract: A precursor lesion to cholangiocarcinoma: Radiol Case Rep. 2019; 14: 495–500.