Introduction
Basal Cell Carcinoma (BCC) is a malignant tumor of the skin originating from the basal layer of the epidermis and its appendages, and is one of the most common malignant tumors in dermatology. The disease is a low-grade malignancy with a slow course of progression. Long-term ultraviolet exposure is one of the most important risk factors, and it is more common in middle-aged and elderly people, especially in sun-exposed areas such as the face and face [1]. There are still many cases of non-exposed parts, such as the neck, trunk, limbs, perineum and perianal areas. The etiology of BCC is complex and may involve multiple factors. In recent years, the incidence of BCC has been on the rise worldwide, threatening the lives and health of patients, so it is necessary to analyze the clinical characteristics and treatment effects of basal cell carcinoma of the skin. This study retrospectively analyzed the clinical data and surgical efficacy of patients with BCC confirmed by biopsy in the Department of Dermatology, Chaohu Hospital, Anhui Medical University from December 2017 - December 2022, and is reported as follows.
Clinical data and ethics
Study design and ethics
In this study, a total of 123 patients with BCC confirmed by pathological biopsy were admitted to our hospital from December 2017 to December 2022. Approved by the Ethics Committee of Chaohu Hospital Affiliated to Anhui Medical University (KYXM 202304-007). We demonstrate that the study was conducted in accordance with the 1964 Declaration of Helsinki and subsequent amendments. Written informed consent was obtained from all participants prior to enrollment in this study.
Clinical data
From December 2017 to December 2022, 123 cases of BCC patients were diagnosed by pathological biopsy in Chaohu Hospital Affiliated to Anhui Medical University. Male 66 cases, female 57 cases, male to female ratio 1.16:1.; age of onset (38~94) years, the average age of onset is (65.58±12.86) years, male and female onset age distribution is not statistically different (χ2=2.116, P>0.05). The duration of consultation was shorter in males (3.10±2.92) than in females (6.10±6.55) years, which was statistically significant (P<0.01).
Table 1: General information about the patient.
| Age (Years) |
Disease |
| Groups |
N |
<40 |
40~59 |
60~79 |
≥80 |
Duration (years) |
| Male |
66 |
1 |
23 |
35 |
7 |
3.10±2.92 |
| Female |
57 |
0 |
16 |
33 |
8 |
6.10±6.55 |
| χ2(t) |
|
2.1160.549 |
3.201 |
| P |
|
0.002 |
Survey on willingness to consult
63 cases of active consultation and 4 cases of passive consultation in the < 60 years old group, with an active consultation rate of 94.03%; 17 cases of active consultation and 39 cases of passive consultation in the ≥60 years old group, with an active consultation rate of 30.36%, and there was a statistically significant difference between the two groups, as shown in (Table 2).
Table 2: Patients’ willingness to attend.
| Groups |
How to visitthe clinic1 |
How to visitthe clinic2 |
Sum |
χ2 |
P |
| <60 |
63(94.03) |
4(5.97) |
67(54.47) |
55.157 |
<0.01 |
| ≥60 |
17(30.36) |
39(69.64) |
56(45.53) |
|
|
| Sum |
80(65.04) |
43(34.96) |
123(100.00) |
|
|
Marginal notes: 1: Seek medical advice on one’s own initiative;
2: Passive inpatient service.
Clinical and pathological types nodular ulcerative type (including nodular or ulcerative type)
88 cases (71.54%), pigmented type: 21 cases (17.07%), sclerotic type 5 cases (4.07%), and others (superficial, fibroepithelioma type, etc.) 8 cases (6.50%). A total of 118 cases (93.06%) were located in the head and face, 3 cases (4.17%) in the trunk, and 2 cases (2.78%) in the limbs, and there was no statistically significant difference in their distribution (χ2=10.235, P>0.05), as shown in Table 3.3. 3 cases had mild pain (2.44%), 4 cases had mild itching and discomfort (3.25%), and 2 cases had both pain and itching (1.63%). The rest had no symptoms.
Misdiagnosis
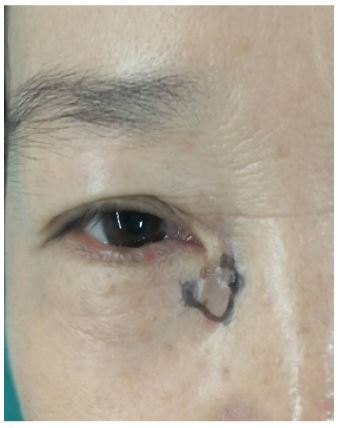
There were 19 cases of misdiagnosis with a misdiagnosis rate of 15.45%. Initial misdiagnosis was made in 4 cases (3.25%), which were seborrheic keratosis in 2 cases (1.63%), squamous carcinoma in 1 case (0.81%) and Bowen’s disease in 1 case (0.81%). Due to non-pigmented type had been misdiagnosed several times in 15 cases (12.20%) as cysts in 9 cases (7.32%) as shown in (Figure 1), as keloids in 2 cases (2.44%) as shown in (Figure 2), as dental fistula in 2 cases (1.63%), as chronic inflammation of lacrimal duct in 1 case as shown in (Figures 3-4), as well as eczema of the ear in 1 case (0.81%) as shown in (Figure 5).
Table 3: Distribution of patients by clinical type.
| Groupsulcer type based |
Nodular |
Pigment |
Sclerotic |
Other types |
Sum |
| Head |
87(73.73) |
19(16.10) |
5(4.24) |
7(5.93) |
118(93.06)face |
| Trunk |
0(0.00) |
2(66.67) |
0(0.00) |
1(33.33) |
3(4.17) |
| Limb |
1(50.00) |
1(50.00) |
0(0.00) |
0(0.00) |
2(2.78) |
| Sum |
88(71.54) |
21(17.07) |
5(4.07) |
8(6.50) |
123(100.00) |
Combination of other diseases
Combined with other skin diseases 16 cases (13.01%). 8 cases of solar keratosis, 2 cases of solar keratosis and squamous skin cancer (Figure 6), 3 cases of psoriasis, 2 cases of urticaria, and 1 case of atopic dermatitis.
Prognosis
One case of superficial type patient was diagnosed by pathology, the family thought that the patient was old and there was no need for treatment, so they gave up the treatment. 1 year later, the tumor appeared to be shedding phenomenon, the black necrotic scabs could be easily pushed away with a little force with a cotton swab, under which was the normal skin, and at present, there was no recurrence in the follow up, see (Figure 7). 2 patients chose to have surgical treatment in overseas hospitals, and the rest of the 120 cases chose to have surgical treatment in our department, among which, 110 cases were completely resected by Mohs surgery for one time, and 9 cases were expanded twice in the operation. complete resection, 9 cases of intraoperative secondary expansion of the resection, 3 cases of patients in the surgical process of the tumor was accidentally cut off, Mohs surgery reference value is affected, so the postoperative monthly combined 2% lidocaine injection 5 ml + Recombinant human Interferon α(INF-α) 100u + 5-Fluorouracil (5-FU) appropriate amount of mixture in the resection area of the local injection treatment, 1 time per month, a total of 3 times; surgical incision open combined photodynamic therapy 2 cases, 1 time per week, a total of 3 times, later change the second stage of healing. All patients did not see recurrence or distant metastasis.
Discussion
BCC is a low-grade malignant skin tumor derived from basal cells with multiple potential differentiation, and the prevalence accounts for 75%-80% of non-melanotic malignant tumors of the skin [2], BCC is a malignant tumor derived from the epidermis or its appendages, especially the basal cells of hair follicles, and is one of the most common malignant tumors in dermatology, which often occurs in elderly men, but the incidence of young people is also increasing year by year. Because long-term sun exposure is one of the important predisposing factors of the disease, BCC is highly prevalent in sun-exposed areas such as the face, hands and feet [3]. In this retrospective study, the male-to-female ratio of patients with BCC was 1.16:1, with approximately more males than females, similar to other reported results [3]. Possible reasons: 1) Men are more engaged in outdoor work than women, and the probability of exposure to ultraviolet light is much higher than that of women [1]; 2) there is growing evidence that non-ultraviolet radiation factors, such as sex hormones, play a protective role in BCC [4]; 3) Older men may pay more attention to personal health, resulting in a higher probability of medical treatment than older women. This study showed that the peak age of medical treatment was 60~80 years old, accounting for 55.28%, and 93.06% were mainly head and face. In foreign studies, 89.50% were over 60 years old, 98.50% were head and neck, and the positive rate of surgical margins was 9%, and the recurrence rate was 1.5% [5]. There are some differences between the two, which may be related to cultural differences, desire to seek medical treatment, health awareness, economic level, geographical environment and other factors.
BCC can invade along the surrounding skin appendage tissues such as sweat glands, skin glands, and hair follicles, and can occur on the basis of certain skin lesions such as actinic keratosis, chronic ulcers, chronic infections, and scar tissue [6], so the clinical manifestations are polymorphic, such as small papules, nodules, and pigmented plaques at first, and black, brown, and dark red skin lesions with no obvious specificity [7,8], so they are easy to be misdiagnosed at the initial diagnosis. Clinically, the diagnosis of cutaneous BCC depends on medical history, clinical characteristics of skin lesions, dermoscopy and skin biopsy histopathological examination, among which dermoscopy can be early identification, effectively reduce the misdiagnosis rate, and have important clinical value for early diagnosis and treatment. However, the gold standard for the diagnosis of cutaneous BCC remains histopathological examination, with nodular ulceration being the most common pathological type, followed by pigmented type, similar to other studies [9,10]. The need for dermoscopy is still supported by the need for dermoscopy as it can detect abnormal skin structures at an early stage and follow up regularly to avoid chances. In this study, a small number of BCC patients with atypical clinical symptoms were misdiagnosed with ear eczema, cysts, keloids, and dental fistulas, so skin biopsy is essential to confirm the diagnosis and assess the risk of the disease. In foreign studies,
30.20% of the cases were misdiagnosed as pigmented nevi [11]. With the popularization and attention of science in China in recent years, cases of misdiagnosis of moles have become very rare. This study shows that most patients have no symptoms, so patients often delay treatment because their symptoms are not obvious and are considered insignificant. However, the results of this study were the opposite, and the active medical treatment rate over 60 years old was significantly lower than that of people under 60 years old, which was statistically significant (P<0.05), suggesting that the older the age, the less attention to skin health, or other concerns such as financial and troublesome children.
BCC can be combined with other skin diseases such as psoriasis, urticaria, and atopic dermatitis, but whether there is a certain association between the two needs to be further investigated [12,13]. Current studies suggest that the pathogenesis of psoriasis, skin fibrosis, scleroderma, BCC, and squamous cell carcinoma may be related to dysregulation of the common pathway, the JNK pathway [14].
BCC is a malignant skin tumor and is not sensitive to radiation, so radiation therapy is generally not recommended [15]. In this study, one patient with superficial type developed self-healing, and the superficial type was relatively good. Surgical excision is currently the most effective treatment for BCC [16], and intralesional injection of 5fluorouracil (5-FU) is an effective alternative or effective means of postoperative salvage in patients who are reluctant to undergo surgery [17,18], and is superior to other chemotherapeutic agents. Recombinant human Interferon Alpha-2b (IFN-α2b) has been successfully used for the intralesional treatment of BCC [19]. Studies have shown that intralesional injection of IFN-α2b in the treatment of BCC is comparable to that of surgery [20,21]. In this study, the integrity of the tumor tissue was destroyed due to a variety of factors during the operation, and it is not very certain that the tumor tissue was completely removed, so skin grafting or open secondary healing should be selected, and an appropriate amount of 2% lidocaine injection 5 ml + IFNα2b 100u + 5-FU 0.25 mg mixture should be injected into the incision every month after 2 weeks, a total of 3 times. In this study, 3 patients were treated with IFN-α combined with 5-FU local injection after surgery, which can be used as a reference. In addition, photodynamic therapy can be used in patients who are able to do so [22-24], and a combination of photodynamic therapy (once a week for a total of three times) during or after surgery is also a good postoperative remedy [21]. In this study, 2 patients were treated with postoperative photodynamic therapy, and both patients achieved satisfactory efficacy. In this study, skin grafting or vacant treatment was used for uncertain surgery, and the treatment effect was satisfactory in combination with other treatments in the later stage.
For the very few cases of advanced and BCC metastases, treatment remains a significant clinical challenge. Recently, it has been reported that Hedgehog signaling inhibitors, such as vemodigib and sonedigil, have been successfully used as targeted therapies for advanced BCC [24,25]. It can be used as a new treatment option. Limitations in this study: The selected cases in this study are patients in or around the region, so this study has a regional nature; Treatment with Hedgehog signaling inhibitors [26,27] has not been tried.
Conclusion
In summary, this study shows that BCC is more common in the face of middle-aged and elderly people, and men are more likely to be misdiagnosed than women, and non-melanogenic BCC is easy to be misdiagnosed. BCC is a benign tumor, and a very small number of patients have self-healing, and no distant metastasis has been found. Surgical complete excision is the best treatment for BCC, and if surgery may be left over, it can be combined with photodynamic and local injection. In the future, it is our common direction to find more convenient and economical treatment methods with a high cure rate of tumors.
Declarations
Data availability statement: The data underlying this article will be shared on reasonable request to the corresponding author.
Conflicts of interest: The authors declare no competing interests.
Data availability statement: The data underlying this article will be shared on reasonable request to the corresponding author.
Authors’ contributions: Haoying Lin: Drafting and editing of the manuscript; review of the bibliography; review of the manuscript; approval of the final version of the manuscript. Minghai Zhang: Effective participation in research orientation; critical review of the literature; critical review of the manuscript; approval of the final version of the manuscript.
Acknowledgements: We would like to give our heartfelt thanks to all participants in this study. In addition, my sincere and hearty thanks and appreciations go firstly to my supervisor, Mr. Zhang Minghai, whose encouragement and suggestions have given me much help in this study. Finally, I am also extremely grateful to all my friends and classmates who have kindly provided me assistance and companionship.
References
- Lashway SG, Worthen ADM, Abuasbeh JN, Harris RB, Farland LV, O’Rourke MK, et al. A meta-analysis of sunburn and basal cell carcinoma risk. Cancer Epidemiol. 2023; 85: 102379.
- Katalinic A, Kunze U, Schafer T. Epidemiology of cutaneous melanoma and non-melanoma skin cancer in schleswig-holstein, germany: incidence, clinical subtypes, tumour stages and localization (epidemiology of skin cancer). Br J Dermatol. 2003; 149: 1200-1206.
- Temel M, Koc MN, Ulutas S, Gogebakan B. The expression levels of the sirtuins in patients with BCC. Tumour Biol. 2016; 37: 6429-6435.
- Collier V, Musicante M, Patel T, Liu-Smith F. Sex disparity in skin carcinogenesis and potential influence of sex hormones. Skin Health Dis. 2021; 1: e27.
- Ozbey R. Basal cell skin cancers: retrospective analysis of 67 cases. J Cosmet Dermatol. 2022; 21: 7007-7012.
- Cohen PR. Basal cell carcinoma associated with non-neoplastic cutaneous conditions: a comprehensive review. Dermatol Online J. 2021; 27.
- Shimada Y, Morita K, Kabasawa Y, Taguchi T, Omura K. Clinical manifestations and treatment for keratocystic odontogenic tumors associated with nevoid basal cell carcinoma syndrome: a study in 25 japanese patients. J Oral Pathol Med. 2013; 42: 275-280.
- Kimonis VE, Goldstein AM, Pastakia B, Yang ML, Kase R, Digiovanna JJ, et al. Clinical manifestations in 105 persons with nevoid basal cell carcinoma syndrome. Am J Med Genet. 1997; 69: 299-308.
- Al-Qarqaz F, Bodoor K, Al-Tarawneh A, Eloqayli H, Al Gargaz W, Alshiyab D, et al. Erratum to «basal cell carcinoma pathology requests and reports are lacking important information. J Skin Cancer. 2019; 2019: 6846428.
- Lasinska I, Zielinska A, Mackiewicz J, Souto EB. Basal cell carcinoma: pathology, current clinical treatment, and potential use of lipid nanoparticles. Cancers (Basel). 2022; 14.
- Tiyawatanaroj A, Sudtikoonaseth P, Chayangsu O. Basal cell carcinoma trends in thailand: a 10-year retrospective study of demographic, clinical and histopathological features. Dermatol Reports. 2022; 14: 9413.
- Spallone G, Sollena P, Ventura A, Fargnoli MC, Gutierrez C, Piccerillo A, et al. Efficacy and safety of vismodegib treatment in patients with advanced basal cell carcinoma and multiple comorbidities. Dermatol Ther. 2019; 32: e13108.
- Reinau D, Surber C, Jick SS, Meier CR. Epidemiology of basal cell carcinoma in the united kingdom: incidence, lifestyle factors, and comorbidities. Br J Cancer. 2014; 111: 203-206.
- Hammouda MB, Ford AE, Liu Y, Zhang JY. The JNK signaling pathway in inflammatory skin disorders and cancer. Cells 2020; 9.
- Abatli S, Hasan M, Sholi SB, Qashoo A, Maqboul I. Recurrent Basal Cell Carcinoma (BCC) of the forearm: a case report. Cureus. 2023; 15: e40247.
- Narayanan K, Hadid OH, Barnes EA. Mohs micrographic surgery versus surgical excision for periocular basal cell carcinoma. Cochrane Database Syst Rev. 2014; 2014: CD007041.
- Maghfour J, Kuraitis D, Murina A. Intralesional 5-fluorouracil for treatment of non-melanoma skin cancer: a systematic review. J Drugs Dermatol. 2021; 20: 192-198.
- Pederson H, Staples CJ, Housewright C. Topical fluorouracil therapy for residual superficial basal cell carcinoma following mohs micrographic surgery. J Drugs Dermatol. 2020; 19: 485-486.
- Dessinioti C, Stratigos AJ. Immunotherapy and its timing in advanced basal cell carcinoma treatment. Dermatol Pract Concept. 2023; 13.
- Maleki M, Layegh P, Kiafar B, Teimoorian M, Darchini-Maragheh E, Razmara M. Treatment of basal cell carcinoma with intralesional interferon alfa-2b: an open-label clinical trial. Expert Rev Anticancer Ther. 2023; 23: 753-760.
- Toma S, Vincenti M, Palumbo R, Muzio G, Rainero M, Santi P, et al. Results of the association of intralesional recombinant alpha-interferon-2a (alpha-IFN) plus 13-cis-retinoic acid (13cra) in the treatment of basal-cell carcinomas (bcc) of the skin. Int J Oncol. 1993; 3: 1149-1154.
- Mazur E, Kwiatkowska D, Reich A. Photodynamic therapy in pigmented basal cell carcinoma-a review. Biomedicines. 2023; 11.
- de Albuquerque IO, Nunes J, Figueiro Longo JP, Muehlmann LA, Azevedo RB. Photodynamic therapy in superficial basal cell carcinoma treatment. Photodiagnosis Photodyn Ther. 2019; 27: 428-432.
- Collier NJ, Rhodes LE. Photodynamic therapy for basal cell carcinoma: the clinical context for future research priorities. Molecules. 2020; 25.
- Fania L, Didona D, Morese R, Campana I, Coco V, Di Pietro FR, et al. Basal cell carcinoma: from pathophysiology to novel therapeutic approaches. Biomedicines .2020; 8.
- Ingham PW. Hedgehog signaling. Curr Top Dev Biol. 2022; 149: 1-58.
- Cai E, Barba MG, Ge X. Hedgehog signaling in cortical development. Cells. 2023; 13.