Introduction
Breast cancer is the most prevalent and leading cause of cancer-related deaths in women [1]. Hormone receptor-positive and human epidermal growth factor receptor 2 (HER2)-negative breast cancer makes up around 66% of all malignant neoplasms in the breast [2-4]. Adjuvant endocrine treatment can effectively treat hormone-receptor positive breast cancer in its early stages. However, a few individuals experienced recurrence or distant metastases due to endocrine treatment resistance. According to the ESMO 5th worldwide consensus recommendations for advanced breast cancer in 2020, primary endocrine resistance (De novo resistance) is defined as recurrence during the first two years of adjuvant ET or Progressive Disease (PD) within the first six months of first-line ET for MBC while on ET. Secondary endocrine resistance is defined as relapse during adjuvant ET but beyond the first 2 years, relapse within 12 months after finishing adjuvant ET, or PD ≥6 months after commencing ET for MBC while on ET [5].
Three CDK4/6 inhibitors have shown promising effects in clinical trials: Palbociclib [6-8], Ribociclib [9-12], and Abemaciclib [13,14]. Clinical trials show that combining CDK4/6 inhibitors with endocrine treatment increases Progression-Free Survival (PFS) over endocrine therapy alone. These drugs are intended to treat hormone receptor-positive, HER2-negative metastatic breast tumors. Palbociclib is utilized as a first-line therapy for postmenopausal women, in conjunction with an aromatase inhibitor [1517].
It is also used in combination with fulvestrant in premenopausal and postmenopausal women who have disease progression after endocrine therapy. Fulvestrant exerts its impact by downregulating and degrading the estrogen receptor. Premenopausal women should have their ovarian function suppressed or ablation during endocrine treatment [8,9].
Ribociclib is used as the initial endocrine treatment in premenopausal and postmenopausal women, with an AI. It is also used in conjunction with fulvestrant as the first endocrine treatment in postmenopausal women, as well as in postmenopausal patients who progress after endocrine therapy [10-12].
Abemaciclib is used as the initial endocrine medicine in postmenopausal women, in combination with an AI. It is also used in conjunction with fulvestrant to treat premenopausal and postmenopausal women whose illness progresses despite endocrine therapy. If the illness continues despite endocrine and chemotherapy treatment, Abemaciclib may be used as a monotherapy if disease progresses on endocrine therapy and chemotherapy [13,14].
These CDK inhibitors are usually well tolerated, while they can have some side effects, as reported here [15,16]. For example, typical adverse effects include tiredness, nausea, neutropenia, and infection, although interstitial lung disease is less prevalent. Ribociclib can also produce QTc prolongation and hepatotoxicity, whereas Abemaciclib can result in hepatotoxicity, increased blood creatinine, and grade 3 diarrhea [17,18].
Although the development and licensure of CDK inhibitors have revolutionized the treatment of metastatic breast cancer, resistance to these drugs has also emerged. As a result, more research into the underlying mechanism of acquired resistance to these drugs is required, as is the development of novel CDK inhibitors. This trial will compare the effect of CDK4/6 plus hormonal treatment on progression-free survival to hormonal treatment alone, as well as the tolerance, effectiveness, and safety profile of CDK4/6 inhibitors when combined with hormonal therapy.
Research methodology & design
Study design
This was a comparative, record-based retrospective cohort study aiming to compare the effectiveness of CDK4/6 with hormonal treatment on progression-free survival to hormonal treatment alone, as well as the tolerance and toxicity profile of CDK4/6 after hormonal therapy.
Study setting
This study was conducted at Suez Canal University Hospital’s (SCUH) Clinical Oncology and Nuclear Medicine Department in Ismailia, Egypt. The patients were identified via the department registry, and data was retrieved from their medical records using a predetermined form.
Patient selection and data collection
The sample size was computed. We gathered all eligible patients from their records within the appropriate timeframe (1/2022 to 6/2024) depending on sample size and monitored them to record disease outcome and clinicopathological features.
Patients are classified into two groups:
• Group A got CDK 4/6 plus hormonal therapy.
• Group B: received hormonal treatment only.
The data for this study came from the Clinical Oncology Department’s patient file recording system. The data obtained included:
• Personal data:
- Age at the time of diagnosis
- Family history of breast cancer.
- Chronic illness is defined as diseases that persist one year or more and need continuing medical treatment, impede everyday activities, or both (according to the Center for Disease Control).
• Clinical data:
- ECOG performance status.
- Menopausal stages include premenopausal, perimenopausal, and postmenopausal.
• Radiological findings
• Pathological data:
- Receptors at the metastatic tumor site (ER and PR receptors)
- Progesterone receptor status.
- Metastatic luminal categorization (Luminal A & B), with Luminal A tumors having the presence of ER and/or PR but no HER2, as well as a low expression of the cell proliferation marker Ki67 (less than 20%). Luminal B tumors are of higher grade and worse prognosis compared to Luminal A. They are ER positive, can be PR negative, and have a high expression of Ki67 (greater than 20%).
- Ki 67 proliferation index.
- Tumor stage at the time of diagnosis.
• First line treatment received:
- First-line adjuvant/neoadjuvant chemotherapy (in case received).
- Type of chemotherapy.
- Adjuvant radiotherapy.
• Adjuvant endocrine therapy:
- First-line hormonal treatment in an adjuvant setting.
- Period of adjuvant endocrine therapy in months.
- Primary endocrine resistance (De novo resistance) is defined as: relapse while on the first 2 years of adjuvant ET. Secondary (acquired) endocrine resistance is defined as: relapse while on adjuvant ET but after the first 2 years.
• Metastasis:
- Timing of metastasis (period of disease-free) indicating number of months from time of presentation till development of metastasis.
- Pattern of metastasis (bone metastasis only, bone and visceral metastasis, bone and non-visceral metastasis, visceral metastasis only (lung, liver, brain), non-visceral only (lymph nodes, skin, other breast), visceral and non-visceral metastasis, bone visceral non-visceral.
- Visceral metastasis defined as lung, liver, and brain metastasis, while non-visceral only (lymph nodes, skin, other breast).
• Number of sites/organs of metastasis.
• Endocrine therapy at the time of metastasis.
• Type of CDK 4/6 inhibitor received (Ribociclib, Abemaciclib, Palbociclib) in Group A.
• Adverse events occurred according to common terminology criteria for adverse events.
• Whether discontinuation of drug due to toxicity occurs & mean time in months, in addition post discontinuation therapy.
• Assessment of treatment response after 6 months of starting treatment. This is according to RECIST criteria.
• Progression-free survival on a CDK4/6 inhibitor or hormonal treatment.
• Status at the date cutoff (alive or dead).
• Overall survival (from date of diagnosis till date cutoff June 2024).
• Compliance on treatment arm either CDK 4/6 inhibitor or hormonal treatment. Patient may be shifted due to toxicity to another CDK 4/6 inhibitor, progressed and shifted to another line, or stay on the same line of treatment at the date cutoff.
• Follow-up data for every patient recorded.
Inclusion criteria:
• Female patients only.
• Age is more than or equal to 20 years old.
• Immunohistochemistry proved metastatic luminal breast cancer patients.
• Radiologically confirmed skeletal, visceral, or non-visceral metastasis.
Exclusion criteria:
• Multiple primary tumors or double pathological lesions.
• Triple-negative breast cancer.
• Her2neu-enriched breast cancer.
• Non-metastatic luminal breast cancer.
• Male breast cancer.
Sample size and sampling technique:
From January 2022 to June 2024, a simple random sample of patients attended the Clinical Oncology and Nuclear Medicine department at Suez Canal University Hospital. We included patients who were diagnosed with metastatic luminal breast cancer using pathology, immunohistochemistry, and radiography. Patients must fulfill the inclusion and exclusion criteria.
Sample size:
The sample size was determined using the following equation [19]:
n = (Zα/2+Zβ)2* (p1 (1-p1) +p2 (1-p2)) / (p1-p2)2
where Zα/2 is the critical value of the Normal distribution at α/2 (e.g. for a confidence level of 95%, α is 0.05 and the critical value is 1.96),
Zβ is the critical value of the Normal distribution at β (e.g. for a power of 80%, β is 0.2 and the critical value is 0.84).
P1 and p2 are the expected sample proportions of the two groups.
P1 was 63% and p2 was 42.2% [20]
The calculated sample size is 174 participants.
Ethical considerations
The research ethics committee of the Faculty of Medicine Suez Canal University (FOMSCU) has approved the final protocol.
Clinical data will be collected with the agreement of FOMSCU’s research ethics council.
The study data will be collected from the patient’s files. To safeguard patient confidentiality and privacy, no personally identifiable information will be released.
The data will only be used for that research; moreover, patient contact will be required to decrease the challenges associated with inaccurate recording and follow-up.
The data analysis will be displayed in a covert way, with no mention of patient identities.
Statistical analysis
The statistical analysis was carried out using SPSS software for Windows, version 28 (IBM Co., Armonk, NY, USA). The MannWhitney or Kruskal-Wallis tests were used to analyze numerical data in the form of median and Interquartile Range (IQR). Categorical data were presented as frequency and percentage, then analyzed using the chi-square or exact test, as appropriate.
The Kaplan-Meier curve with log-rank test was used for survival analysis, and Cox regression was used to investigate various survival factors. A two-tailed P value<0.05 indicates statistical significance.
Results
Baseline patient characteristics
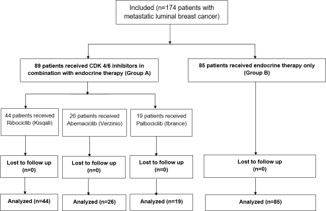
From January 2022 to June 2024, 174 people were tested for eligibility at the Clinical Oncology and Nuclear Medicine departments at Suez Canal University Hospital. Each of these individuals had metastatic luminal breast cancer. Of those, 89 patients received Cdk 4/6 inhibitors in addition to endocrine therapy and were assigned to Group A, whereas 85 patients received just endocrine therapy and were assigned to Group B. (Table 1) provides a complete description of the baseline patient characteristics. There was no significant difference in baseline patients between the two therapy groups in terms of age, family history, comorbidities, menopausal state, or ki-67 proliferation index. There was only a difference in tumor stage and ECOG PS at the time of diagnosis (P value=0.030 and 0.001, respectively). Metastatic luminal categorization at the time of metastasis differs between the two groups (p value=0.007).
Table 1: Baseline characteristics of the studied groups.
| Item |
|
Group A (n=89) |
Group B (n=85) |
P-value |
| Age group (years) |
20-29 |
1(1.1%) |
0(0%) |
0.360 |
| 30-39 |
6(6.7%) |
7(8.2%) |
| 40-49 |
19(21.3%) |
17(20%) |
| 50-59 |
42(47.2%) |
29(34.1%) |
| 60-69 |
18(20.2%) |
26(30.6%) |
| 70-79 |
3(3.4%) |
5(5.9%) |
| 80-89 |
0(0%) |
1(1.2%) |
| ECOG performance |
PS1 |
85(95.5%) |
67(78.8%) |
0.001 |
| PS2 |
4(4.5%) |
18(21.2%) |
| Family history |
|
2(2.2%) |
6(7.1%) |
0.161 |
| Comorbidities |
No chronic illness |
65(73%) |
59(69.4%) |
0.526 |
| HTN |
7(7.9%) |
11(12.9%) |
| DM |
6(6.7%) |
7(8.2%) |
| Chronic liver disease |
1(1.1%) |
2(2.4%) |
| Asthma |
2(2.2%) |
0(0%) |
| Cardiac disease |
1(1.1%) |
2(2.4%) |
| HTN & DM |
0(0%) |
1(1.2%) |
| Others |
7(7.9%) |
3(3.5%) |
| Menopausal status |
Premenopausal |
19(21.3%) |
20(23.5%) |
0.248 |
| Perimenopausal |
7(7.9%) |
13(15.3%) |
| Postmenopausal |
63(70.8%) |
52(61.2%) |
| Receptors at metastatic site |
ER and PR both positive |
87(97.8%) |
83(97.6%) |
>0.999 |
| ER positive |
2(2.2%) |
2(2.4%) |
| Progesterone receptor status |
Positive |
87(97.8%) |
83(97.6%) |
>0.999 |
| Negative |
2(2.2%) |
2(2.4%) |
| Metastasis luminal lassification |
Luminal A |
28(31.5%) |
44(51.8%) |
0.007 |
| Luminal B |
61(68.5%) |
41(48.2%) |
| KI-67 (%) |
|
30(10, 40) |
20(10, 40) |
0.159 |
| Tumor stage at time of presentation |
Stage 1 |
3(3.4%) |
9(10.6%) |
0.030 |
| Stage 2 |
33(37.1%) |
30(35.3%) |
| Stage 3 |
34(38.2%) |
39(45.9%) |
| Stage 4 |
19(21.3%) |
7(8.2%) |
Numerical data are presented as median (IQR) and categorical data are presented as frequency (%), Statistical significance at P value<0.05.
ECOG: Eastern Cooperative Oncology Group; PS: Performance Status; HTN: Hypertension; DM: Diabetes Mellitus; ER: Estrogen Receptor; PR: Progesterone Receptor
First-line treatment details
In group A, 66 patients (74.2%) were given first-line chemotherapy (59.6% anthracycline and taxanes, 14.6% taxanes alone) in the adjuvant/neoadjuvant setting. In group B, 62 patients got first-line chemotherapy, with 48.2% receiving anthracycline plus taxanes and 24.7% receiving taxanes alone, with a statistically insignificant P value.
The duration of adjuvant endocrine treatment (in months) was considerably shorter in group A than in group B (P=0.002), with a median of 60 (IQR 24, 67.5) versus 60 (IQR 60, 84). The majority of patients in groups A and B got aromatase inhibitors as their first line hormonal therapy in the adjuvant context (44.9% and 47.1%, respectively), followed by LHRH with AI (16.9% and 30.6%). 27.3% of the study population was metastatic from the start and did not receive adjuvant endocrine therapy, while 3.5% presented with primary triple negative breast cancer at the primary tumor site and were later diagnosed with metastatic luminal breast cancer via immunohistochemistry (this is why they did not receive adjuvant hormonal therapy). Table 2 illustrates the first line of therapy received.
Table 2: First line treatment of the studied groups.
| Item |
Group A |
Group B |
P-value |
| (n=89) |
(n=85) |
| First line chemotherapy in adjuvant/neoadjuvant setting |
66(74.2%) |
62(72.9%) |
0.856 |
| Type of chemotherapy |
Anthracycline and Taxane based chemotherapy |
53(59.6%) |
41(48.2%) |
0.19 |
| Taxane based chemotherapy only |
13(14.6%) |
21(24.7%) |
|
| Didn’t receive 1st line chemotherapy |
23(25.8%) |
23(27.1%) |
|
| Adjuvant radiotherapy on breast or chest wall |
66(74.2%) |
68(80%) |
0.36 |
| Period of adjuvant endocrine therapy (months) |
60(24, 67.5) |
60(60, 84) |
0.002 |
| First line hormonal treatment in adjuvant setting |
Antiestrogen |
9(10.1%) |
11(12.9%) |
0.006 |
| Aromatase inhibitor |
40(44.9%) |
40(47.1%) |
|
| LHRH analogue plus antiestrogen |
6(6.7%) |
0(0%) |
|
| LHRH analogue plus AI |
15(16.9%) |
26(30.6%) |
|
| Metastatic from the start |
18(20.2%) |
6(7.1%) |
|
| Did not received 1st line hormonal |
1(1.1%) |
2(2.4%) |
|
| Time to metastasis (months) |
72(36, 96) |
108(72, 123) |
<0.001 |
| Endocrine therapy resistance (adjuvant setting)
| Denovo resistance (primary endocrine therapy resistance) |
22(24.7%) |
11(12.9%) |
0.004 |
| Secondary resistance |
47(52.8%) |
65(76.5%) |
|
| Metastatic from the start |
19(21.3%) |
7(8.2%) |
|
| Did not receive adjuvant endocrine treatment |
1(1.1%) |
2(2.4%) |
|
| Pattern of metastasis development
| Bone metastasis only |
29(32.6%) |
38(44.7%) |
0.247 |
| Bone and visceral |
20(22.5%) |
19(22.4%) |
|
| Bone and non-visceral |
10(11.2%) |
2(2.4%) |
|
| Visceral only (lung, liver, brain) |
10(11.2%) |
11(12.9%) |
|
| Non visceral only (lymph nodes, skin, other breast) |
8(9%) |
8(9.4%) |
|
| Visceral and non-visceral |
4(4.5%) |
2(2.4%) |
|
| Bone, visceral and non-visceral |
8(9%) |
5(5.9%) |
|
| Number of sites / organs of metastasis |
One site |
36(40.4%) |
28(32.9%) |
0.089 |
| Two sites |
34(38.2%) |
46(54.1%) |
|
| Three or more sites |
19(21.3%) |
11(12.9%) |
|
| Endocrine therapy in time of metastasis |
CDK 4/6 inhibitors plus Fulvestrant |
67(75.3%) |
0(0%) |
<0.001 |
| CDK 4/6 inhibitors plus AI |
22(24.7%) |
0(0%) |
|
| Aromatase inhibitor (+ or – LHRH analogue) |
0(0%) |
45(52.9%) |
|
| Aromatase inhibitor and Fulvestrant |
0(0%) |
31(36.5%) |
|
| Fulvestrant alone |
0(0%) |
9(10.6%) |
|
| CDK 4/6 inhibitor subtype |
Ribociclib |
43(48.3%) |
0(0%) |
<0.001 |
| Abemaciclib |
27(30.3%) |
0(0%) |
|
| Palbociclib |
19(21.3%) |
0(0%) |
|
| Did not receive CDK 4/6 inhibitors |
0(0%) |
85(100%) |
|
Numerical data are presented as median (IQR) and categorical data are presented as frequency (%), Statistical significance at P value<0.05.
LHRH: Luteinizing Hormone-Releasing Hormone.
Metastasis
Time to metastasis (months) was considerably shorter in group A compared to group B (P<0.001), with a median of 72 (IQR 36, 96) versus 108 (IQR 72, 123) months. The majority of patients (52.8% of group A vs. 76.5% of group B) acquired secondary endocrine treatment resistance, with a statistically significant difference (P value=0.004). 26 individuals were metastatic from the beginning and did not get adjuvant endocrine therapy. Three individuals tested triple negative at the initial tumor location and did not receive adjuvant hormone treatment.
The majority of patients in groups A and B received aromatase inhibitors as their first-line hormonal treatment in the adjuvant setting (44.9% and 47.1%, respectively), followed by LHRH with AI (16.9% and 30.6%). 27.3% of the study population was metastatic from the start and did not receive adjuvant endocrine therapy, while 3.5% had primary triple negative breast cancer at the primary tumor site but were later diagnosed with metastatic luminal breast cancer via immunohistochemistry. Table 2 illustrates this in detail.
Cdk 4/6 inhibitor plus hormonal treatment versus hormonal alone: In group A, 75.3% received a CDK 4/6 inhibitor in addition to fulvestrant, whereas 24.7% received a CDK 4/6 inhibitor plus aromatase inhibitors. Regarding Cdk 4/6 inhibitors, 48.3% of patients took Ribociclib, 30.3% received Abemaciclib, and 21.3% received Palbociclib.
In group B, patients only got hormonal therapy. 52.9% of patients received both an aromatase inhibitor and LHRH analogues. Others received an aromatase inhibitor with fulvestrant (36.5%) or only fulvestrant (10. 6%). Table 2 illustrates this in detail.
Group A had significantly higher rates of diarrhea (18% vs. 0%, P<0.001), neutropenia (28.1% vs. 0%, P<0.001), easy fatigability (27% vs. 1.2%, P<0.001), abdominal pain (12.4% vs. 0%, P=0.001), anemia (7.9% vs. 0%, P=0.014), arthralgia (33.7% vs. 8.2%, P<0.001), and muscle weakness (6.7% vs. 0%, P=0.029). In contrast, no patients in group A had osteoporosis, but 7.1% of those in group B did, indicating a statistically significant difference between groups (P=0.012). In terms of increased liver enzymes, 4.5% of group A had levels 3 to 5 times higher than normal, whereas 7.1% of group B had levels less than 3 times normal, indicating a statistically significant difference (P=0.002) (Table 3).
Table 3: Adverse events in the studied groups.
| Item |
Group A (n=89) |
Group B (n=85) |
P-value |
| Diarrhea |
Grade 1&2 |
7(7.9%) |
0(0%) |
<0.001 |
| Grade 3 |
9(10.1%) |
0(0%) |
| No |
73(82%) |
85(100%) |
| Neutropenia |
Grade 1&2 |
17(19.1%) |
0(0%) |
<0.001 |
| Grade 3 |
7(7.9%) |
0(0%) |
| Grade 4 |
1(1.1%) |
0(0%) |
| No |
64(71.9%) |
85(100%) |
| Nausea & vomiting |
Grade 3 |
3(3.4%) |
0(0%) |
0.246 |
| No |
86(96.6%) |
85(100%) |
| Easy fatigability |
Grade 1&2 |
20(22.5%) |
1(1.2%) |
<0.001 |
| Grade 3 |
4(4.5%) |
0(0%) |
| No |
65(73%) |
84(98.8%) |
| Abdominal pain |
Grade 1&2 |
10(11.2%) |
0(0%) |
0.001 |
| Grade 3 |
1(1.1%) |
0(0%) |
| No |
78(87.6%) |
85(100%) |
| Anemia |
7(7.9%) |
0(0%) |
0.014 |
| Thrombocytopenia |
2(2.2%) |
0(0%) |
0.497 |
| Febrile neutropenia |
Grade 1&2 |
1(1.1%) |
0(0%) |
0.497 |
| Grade 3 |
2(2.2%) |
0(0%) |
| No |
86(96.6%) |
85(100%) |
| Decreased appetite |
Grade 1&2 |
4(4.5%) |
0(0%) |
0.060 |
| Grade 3 |
2(2.2%) |
0(0%) |
| No |
83(93.3%) |
85(100%) |
| Headache |
|
2(2.2%) |
2(2.4%) |
>0.999 |
| Stomatitis |
Grade 1&2 |
4(4.5%) |
0(0%) |
0.121 |
| Grade 3 |
1(1.1%) |
0(0%) |
| No |
84(94.4%) |
85(100%) |
| Elevated liver enzymes |
Less than 3 fold ULN normal level |
0(0%) |
6(7.1%) |
0.002 |
| From 3 to 5 fold normal level |
4(4.5%) |
0(0%) |
| More than or equal to 5 fold normal level |
1(1.1%) |
0(0%) |
| No elevated liver enzymes |
84(94.4%) |
79(92.9%) |
| Arthralgia |
30(33.7%) |
7(8.2%) |
<0.001 |
| Elevated serum creatinine (renal impairment) |
5(5.6%) |
1(1.2%) |
0.211 |
| Dizziness |
1(1.1%) |
1(1.2%) |
>0.999 |
| Cardiac ECG changes |
1(1.1%) |
0(0%) |
>0.999 |
| Cardiac EF decrease |
2(2.2%) |
0(0%) |
0.497 |
| Muscle weakness |
6(6.7%) |
0(0%) |
0.029 |
| Rash, hot flush |
4(4.5%) |
0(0%) |
0.121 |
| Bony aches |
7(7.9%) |
5(5.9%) |
0.606 |
| Extremity pain |
2(2.2%) |
2(2.4%) |
>0.999 |
| Skin patches |
3(3.4%) |
1(1.2%) |
0.621 |
| Vitiligo |
1(1.1%) |
0(0%) |
>0.999 |
| Osteoporosis |
0(0%) |
6(7.1%) |
0.012 |
| Dry skin |
2(2.2%) |
1(1.2%) |
>0.999 |
| Urinary tract infection |
1(1.1%) |
0(0%) |
>0.999 |
| Vaginal infection |
2(2.2%) |
0(0%) |
0.497 |
| Autoimmune hepatitis |
1(1.1%) |
0(0%) |
>0.999 |
| Acute kidney injury with dialysis need |
1(1.1%) |
0(0%) |
>0.999 |
| Itching and urticarial reaction |
2(2.2%) |
0(0%) |
0.497 |
| Eczema |
1(1.1%) |
0(0%) |
>0.999 |
| Dental pain |
1(1.1%) |
0(0%) |
>0.999 |
| Urinary tract infection |
3(3.4%) |
0(0%) |
0.246 |
| Weight decreased |
2(2.2%) |
0(0%) |
0.497 |
| No other adverse events |
54(60.7%) |
71(83.5%) |
0.001 |
| Hepatobiliary toxic events |
Less than 1.5 ULN |
3(3.4%) |
0(0%) |
0.246 |
| More than 3 - 10 ULN |
1(1.1%) |
0(0%) |
| Normal blood bilirubin level |
85(95.5%) |
85(100%) |
Table 4: Discontinuation to therapy and response of the studied groups.
| Item |
Group A (n=89) |
Group B (n=85) |
P-value |
| Discontinuation due to toxicity |
17 (19.1%) |
0 (0%) |
<0.001 |
| Time to discontinuation (months) |
5 (4, 6) |
|
|
| Status |
Shifted due to toxicity |
15 (16.9%) |
0 (0%) |
<0.001 |
| Progressed |
15 (16.9%) |
52 (61.2%) |
| Still on treatment |
59 (66.3%) |
33 (38.8%) |
| Post discontinuation therapy |
Another CDK 4/6 and hormonal therapy (group A) |
15 (16.9%) |
0 (0%) |
<0.001 |
| Was on hormonal and shifted to CDK 4/6 |
0 (0%) |
40 (47.1%) |
| Chemotherapy |
10 (11.2%) |
8 (9.4%) |
| Best supportive care |
0 (0%) |
3 (3.5%) |
| Everolimus based therapy |
5 (5.6%) |
1 (1.2%) |
| No progression and still on treatment |
59 (66.3%) |
33 (38.8%) |
| Duration on post discontinuation therapy (months) |
4 (3, 22.25) |
12 (6, 23.5) |
0.003 |
| Response according to RECIST criteria after 2nd line treatment |
CR |
21 (23.6%) |
5 (5.9%) |
<0.001 |
| PR |
47 (52.8%) |
38 (44.7%) |
| SD |
13 (14.6%) |
29 (34.1%) |
| PD |
8 (9%) |
13 (15.3%) |
Numerical data are presented as median (IQR) and categorical data are presented as frequency (%), Statistical significance at P value<0.05.
CR: Complete Response; PR: Partial Response; SD: Stationary Disease; PD: Progressive Disease Coarse; RECIST: Response Evaluation
Criteria in Solid Tumors.
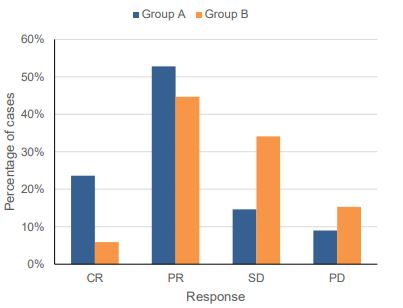
After 6-month treatment, patients in group A shown a considerably greater treatment response than those in group B (P<0.001), with 23.6% showing CR, 52.8% showing PR, 14.6% showing SD, and 9% showing PD compared to 5.9% of the latter (Table 4 & Figure 2).
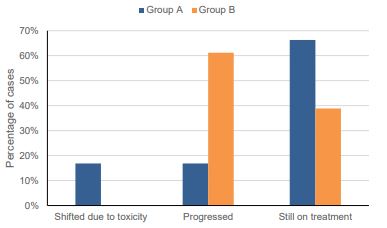
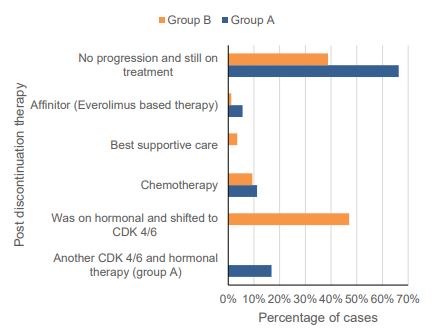
In group A, 19.1% of patients stopped CDK 4/6 owing to toxicity. The average period of discontinuance was 5 months. Furthermore, 16.9% of group A switched to a different line of treatment due to toxicity, whereas 61.2% of group B suffered disease progression and 66.3% remained on the same line of treatment. The difference in proportions between groups was statistically significant (P<0.001) (Table 4 & Figures 3,4).
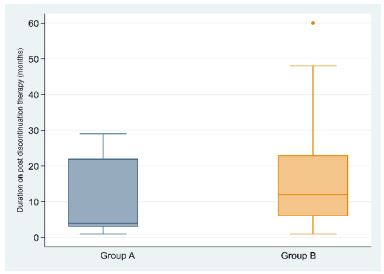
In terms of post-discontinuation therapy, in group A, 16.9% shifted to another CDK 4/6 inhibitor and hormonal therapy with an acceptable toxicity profile, 11.2% of patients developed a visceral crisis and received chemotherapy, and 5.6% received Everolimus-based therapy, whereas in group B, 47.1% were on hormonal therapy and shifted to the other treatment arm, 9.4% received chemotherapy, 3.5% had the best supportive care, and 1.2% had Everolimus-based therapy, indicating Patients in group A got post-discontinuation medication for a median of 4 (IQR 3, 22.25) months, which was significantly less than the time in group B (12 (IQR 6, 23.5) months); P=0.003 (Table 4 & Figure 5).
Table 5: PFS analysis of patients according to treatment method.
| |
N of events (%) |
N Censored (%) |
Mean (95%CI) |
HR (95%CI) |
Log-rank P-value |
| Group A (n=89) |
15 (16.9%) |
74 (83.1%) |
65.53 (54.73 to 76.34) |
0.24 (0.14 to 0.4) |
<0.001 |
| Group B (n=85) |
52 (61.2%) |
33 (38.8%) |
24.52 (18.96 to 30.07) |
Ref |
CI: Confidence Interval; HR: Hazard Ratio.
Statistical significance at P value<0.05.
Survival analysis
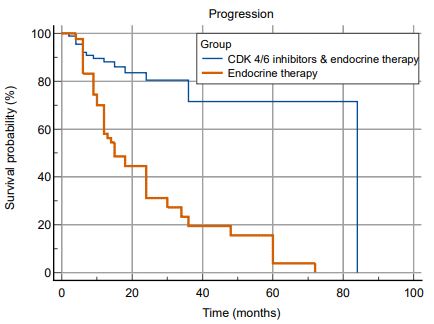
The Kaplan-Meier analysis with log-rank test revealed a statistically significant difference in PFS between the two treatment arms (P<0.001). Patients who received CDK 4/6 inhibitors in combination with endocrine therapy had a longer PFS than those who received endocrine therapy alone, with an estimated mean of 65.53 months (95% CI: 54.73 to 76.34) vs. 24.52 months (95% CI: 18.96 to 30.07), resulting in an incidence rate of 16.9% vs. 61.2%, with an HR of 0.24 (95% CI: 0.14 to 0.4) (Table 5 & Figure 6).
Table 6: OS analysis of patients according to treatment method.
| |
N of events (%) |
N Censored (%) |
Mean (95%CI) |
HR (95%CI) |
Log-rank P-value |
| Group A (n=89) |
2 (2.2%) |
87 (97.8%) |
225.27 (206.3 to 244.25) |
0.82 (0.14 to 4.87) |
0.824 |
| Group B (n=85) |
3 (3.5%) |
82 (96.5%) |
197.06 (189.35 to 204.77) |
Ref |
|
CI: Confidence interval; HR: Hazard Ratio.
Statistical significance at P value<0.05
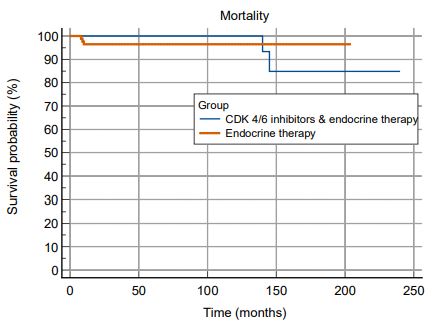
In terms of OS, there was no statistically significant difference between patients in both treatment groups, with death rates of 2.2% and 3.5%, respectively (Table 6 & Figure 7).
In univariate Cox regression analysis, metastasis luminal classification, CDK 4/6 subtype, adverse event exposure, and drug discontinuation due to high toxicity profile were significant predictors of longer PFS, with women with luminal B cancers having a lower risk than those with luminal A subtype (HR=0.53; 95% CI: 0.32 to 0.87, P=0.011). Upon analysis, patients in group A had a substantially decreased risk of tumor progression, with HR (95% CI) of 0.34 (0.17 to 0.68, P=0.002), 0.1 (0.02 to 0.39, P=0.001), and 0.19 (0.05 to 0.79, P=0.023).
Furthermore, individuals who encountered adverse events had a decreased risk of tumor progression compared to those who did not (HR=0.56, 95% CI: 0.34 to 0.92, P=0.021).
Patients who terminated medication owing to toxicity had a substantially reduced risk of progression than others (HR=0.1, 95% CI: 0.01-0.76, P=0.026). Furthermore, patients who received Ribociclib and Abemaciclib had a significantly lower risk of tumor progression than those who received Palbociclib, with HR (95% CI) of 0.26 (0.12 to 0.6, P=0.002) and 0.1 (0.02 to 0.47, P=0.003), respectively (Table 7).
Table 7: Cox-regression analysis for factors associated with PFS of patients.
| Item |
|
Univariate analysis |
Multivariable analysis |
| HR |
95%CI |
P-value |
HR
| 95%CI |
P-value |
| Age group (years) |
20 – 39 |
Ref |
|
|
Ref |
|
|
| 40 – 49 |
0.81 |
0.33 to 1.96 |
0.636 |
0.49 |
0.18 to 1.34 |
0.164 |
| 50 – 59 |
0.42 |
0.18 to 1 |
0.051 |
0.3 |
0.11 to 0.81 |
0.017 |
| 60 – 69 |
0.46 |
0.19 to 1.13 |
0.090 |
0.22 |
0.08 to 0.61 |
0.004 |
| 70 – 89 |
0.7 |
0.14 to 3.38 |
0.655 |
0.36 |
0.07 to 2 |
0.243 |
| Comorbidities (+ve) |
0.88 |
0.5 to 1.55 |
0.660 |
|
|
|
| Metastasis luminal classification |
Luminal A |
Ref |
|
|
Ref |
|
|
| Luminal B |
0.53 |
0.32 to 0.87 |
0.011 |
0.72 |
0.4 to 1.29 |
0.267 |
| KI67 (%) |
0.99 |
0.98 to 1.01 |
0.454 |
|
|
|
| Tumor stage at time of presentation |
Stage 1 |
Ref |
|
|
|
|
|
| Stage 2 |
0.82 |
0.31 to 2.16 |
0.691 |
|
|
|
| Stage 3 |
0.64 |
0.24 to 1.69 |
0.371 |
|
|
|
| Stage 4 |
0.69 |
0.23 to 2.08 |
0.514 |
|
|
|
| First line chemotherapy in adjuvant/neoadjuvant setting |
0.83 |
0.48 to 1.46 |
0.526 |
|
|
|
| Type of chemotherapy |
Didn’t receive 1st line chemotherapy |
Ref |
|
|
|
|
|
| Anthracycline and Taxane based chemotherapy |
0.93 |
0.52 to 1.66 |
0.806 |
|
|
|
| Taxane based chemotherapy only |
0.63 |
0.3 to 1.32 |
0.220 |
|
|
|
| Endocrine therapy resistance in adjuvant setting |
Did not receive adjuvant endocrine treatment |
Ref |
|
|
Ref |
|
|
| Denovo resistance |
0.2 |
0.02 to 1.64 |
0.134 |
0.23 |
0.03 to 2.05 |
0.188 |
| Secondary resistance |
0.3 |
0.04 to 2.26 |
0.243 |
0.34 |
0.04 to 2.76 |
0.316 |
| Metastatic from the start |
0.27 |
0.03 to 2.16 |
0.215 |
0.49 |
0.05 to 4.43 |
0.527 |
| Number of sites/ organs of metastasis |
1.15 |
0.81 to 1.63 |
0.438 |
|
|
|
| CDK 4/6 inhibitor subtype |
No CDK 4/6 |
Ref |
|
|
Ref |
|
|
| Ribociclib (Kisqali) |
0.34 |
0.17 to 0.68 |
0.002 |
0.26 |
0.12 to 0.6 |
0.002 |
| Abemaciclib (Verzinio) |
0.1 |
0.02 to 0.39 |
0.001 |
0.1 |
0.02 to 0.47 |
0.003 |
| Palbociclib (Ibrance) |
0.19 |
0.05 to 0.79 |
0.023 |
0.23 |
0.04 to 1.21 |
0.083 |
| Adverse events |
0.56 |
0.34 to 0.92 |
0.021 |
1.51 |
0.81 to 2.83 |
0.197 |
| Discontinuation due to toxicity |
0.1 |
0.01 to 0.76 |
0.026 |
0.3 |
0.04 to 2.41 |
0.260 |
HR: Hazard ratio, CI: Confidence interval. Statistical significance at P value<0.05
CDK 4/6 inhibitor subtypes
In group A, there was a statistically significant difference in adverse events between the CDK 4/6 inhibitor subtypes. Diarrhea was more common with Abemaciclib, with 34.6% experiencing grade 3 diarrhea with a statistically significant p-value (P-value<0.001). Neutropenia emerged in 36.3% of patients on Ribociclib, followed by Palbociclib (31.6%) and Abemaciclib (11.5%), with a statistically significant difference (P=0.029). 23.1% of Abemaciclib-treated patients had anemia with a hemoglobin level of less than or equal to 9 gm/dL (P=0.003).
Serum creatinine levels increased in 15.4% of Abemaciclib patients (P=0.031). Abemaciclib and Ribociclib caused bone pains in 19.2% and 4.5% of patients, respectively, with a significant P value (P=0.026). Table 8 shows adverse outcomes for CDK 4/6 subtypes.
In terms of medication adherence in Group A, therapy was discontinued due to toxicity in an identical percentage across CDK 4/6 inhibitor subtypes (15.9% with Ribociclib, 15.4% with Abemaciclib, and 21.1% with Palbociclib). The mean time to cessation in months for Ribociclib, Abemaciclib, and Palbociclib was 5.5, 4, and 5 months, respectively.
After 6 months on CDK 4/6 inhibitors, 15 patients had disease progression and failure, whereas 59 stayed on the same treatment group. Patients in Group A were switched to a different treatment line due to unacceptable toxicity or disease progression, as judged by RECIST criteria. Following discontinuation, another CDK 4/6 and hormonal treatment (52.4%) was taken, followed by chemotherapy for a visceral crisis (28.7%) and Everolimus-based therapy (16%). There were no significant differences between CDK 4/6 inhibitor subtypes in terms of therapy response evaluation using RECIST criteria. This is seen in Table 9.
Table 8: Adverse events in group A according to CDK 4/6 inhibitors subtype.
| Item |
CDK 4/6 subtype |
P-value |
| Ribociclib (n=44) |
Abemaciclib (n=26) |
Palbociclib (n=19) |
| Diarrhea |
Grade 1&2 |
0 (0%) |
5 (19.2%) |
2 (10.5%) |
<0.001 |
| Grade 3 |
0 (0%) |
9 (34.6%) |
0 (0%) |
| No |
44 (100%) |
12 (46.2%) |
17 (89.5%) |
| Neutropenia |
Grade 1&2 |
13 (29.5%) |
2 (7.7%) |
2 (10.5%) |
0.029 |
| Grade 3 |
2 (4.5%) |
1 (3.8%) |
4 (21.1%) |
| Grade 4 |
1 (2.3%) |
0 (0%) |
0 (0%) |
| No |
28 (63.6%) |
23 (88.5%) |
13 (68.4%) |
| Nausea & vomiting |
Grade 3 |
0 (0%) |
3 (11.5%) |
0 (0%) |
0.031 |
| No |
44 (100%) |
23 (88.5%) |
19 (100%) |
| Easy fatigability |
Grade 1&2 |
7 (15.9%) |
10 (38.5%) |
3 (15.8%) |
0.021 |
| Grade 3 |
1 (2.3%) |
3 (11.5%) |
0 (0%) |
| No |
36 (81.8%) |
13 (50%) |
16 (84.2%) |
| Abdominal pain |
Grade 1&2 |
4 (9.1%) |
6 (23.1%) |
0 (0%) |
0.075 |
| Grade 3 |
1 (2.3%) |
0 (0%) |
0 (0%) |
| No |
39 (88.6%) |
20 (76.9%) |
19 (100%) |
| Anaemia |
1 (2.3%) |
6 (23.1%) |
0 (0%) |
0.003 |
| Thrombocytopenia |
0 (0%) |
2 (7.7%) |
0 (0%) |
0.127 |
| Febrile neutropenia |
Grade 1&2 |
0 (0%) |
1 (3.8%) |
0 (0%) |
0.085 |
| Grade 3 |
0 (0%) |
2 (7.7%) |
0 (0%) |
| No |
44 (100%) |
23 (88.5%) |
19 (100%) |
| Decreased appetite |
Grade 1&2 |
4 (9.1%) |
0 (0%) |
0 (0%) |
0.052 |
| Grade 3 |
0 (0%) |
2 (7.7%) |
0 (0%) |
| No |
40 (90.9%) |
24 (92.3%) |
19 (100%) |
| Headache |
|
2 (4.5%) |
0 (0%) |
0 (0%) |
0.494 |
| Stomatitis |
Grade 1&2 |
0 (0%) |
2 (7.7%) |
2 (10.5%) |
0.092 |
| Grade 3 |
0 (0%) |
1 (3.8%) |
0 (0%) |
| No |
44 (100%) |
23 (88.5%) |
17 (89.5%) |
| Elevated liver enzymes |
From 3 to 5 fold normal level |
2 (4.5%) |
2 (7.7%) |
0 (0%) |
0.426 |
| More than or equal to 5 fold normal level |
0 (0%) |
1 (3.8%) |
0 (0%) |
| No elevated liver enzymes |
42 (95.5%) |
23 (88.5%) |
19 (100%) |
| Arthralgia |
13 (29.5%) |
9 (34.6%) |
8 (42.1%) |
0.622 |
| Elevated serum creatinine (renal impairment) |
1 (2.3%) |
4 (15.4%) |
0 (0%) |
0.031 |
| Dizziness |
0 (0%) |
1 (3.8%) |
0 (0%) |
0.506 |
| Cardiac ECG changes |
1 (2.3%) |
0 (0%) |
0 (0%) |
>0.999 |
| Cardiac EF decrease |
2 (4.5%) |
0 (0%) |
0 (0%) |
0.494 |
| Muscle weakness |
1 (2.3%) |
2 (7.7%) |
3 (15.8%) |
0.138 |
| Rash, hot flush |
3 (6.8%) |
0 (0%) |
1 (5.3%) |
0.430 |
| Bony aches |
2 (4.5%) |
5 (19.2%) |
0 (0%) |
0.026 |
| Extremity pain |
0 (0%) |
2 (7.7%) |
0 (0%) |
0.127 |
| Skin patches |
3 (6.8%) |
0 (0%) |
0 (0%) |
0.308 |
| Vitiligo |
1 (2.3%) |
0 (0%) |
0 (0%) |
>0.999 |
| Dry skin |
2 (4.5%) |
0 (0%) |
0 (0%) |
0.494 |
| Urinary tract infection |
1 (2.3%) |
0 (0%) |
0 (0%) |
>0.999 |
| Vaginal infection |
2 (4.5%) |
0 (0%) |
0 (0%) |
0.494 |
| Autoimmune hepatitis |
0 (0%) |
1 (3.8%) |
0 (0%) |
0.506 |
| Acute kidney injury with dialysis need |
0 (0%) |
1 (3.8%) |
0 (0%) |
0.506 |
| Itching and urticarial reaction |
2 (4.5%) |
0 (0%) |
0 (0%) |
0.494 |
| Eczema |
1 (2.3%) |
0 (0%) |
0 (0%) |
>0.999 |
| Dental pain |
1 (2.3%) |
0 (0%) |
0 (0%) |
>0.999 |
| Urinary tract infection |
3 (6.8%) |
0 (0%) |
0 (0%) |
0.308 |
| Weight decreased |
1 (2.3%) |
1 (3.8%) |
0 (0%) |
>0.999 |
| No other adverse events |
25 (56.8%) |
14 (53.8%) |
15 (78.9%) |
0.179 |
| Hepatobiliary toxic events |
Less than 1.5 ULN |
1 (2.3%) |
2 (7.7%) |
0 (0%) |
0.320 |
| More than 3-10 ULN |
0 (0%) |
1 (3.8%) |
0 (0%) |
| Normal blood bilirubin level |
43 (97.7%) |
23 (88.5%) |
19 (100%) |
Numerical data are presented as median (IQR) and categorical data are presented as frequency (%), Statistical significance at P value<0.05, EF: Ejection fraction.
Table 9: Discontinuation to therapy and response of group A according to CDK 4/6 inhibitors subtype.
| Item |
CDK 4/6 subtype |
P-value |
| Ribociclib (n=44) |
Abemaciclib (n=26) |
Palbociclib (n=19) |
| Discontinuation due to toxicity |
7 (15.9%) |
4 (15.4%) |
4 (21.1%) |
>0.999 |
| Time to discontinuation (months) |
5.5 (4, 10.5) |
4 (2.5, 5.5) |
5 (5, 5) |
0.247 |
| Status |
Shifted due to toxicity |
7 (15.9%) |
4 (15.4%) |
4 (21.1%) |
0.700 |
| Progressed |
10 (22.7%) |
3 (11.5%) |
2 (10.5%) |
| Still on treatment |
27 (61.4%) |
19 (73.1%) |
13 (68.4%) |
| Post discontinuation therapy |
Another CDK 4/6 and hormonal therapy (group A) |
7 (15.9%) |
4 (15.4%) |
4 (21.1%) |
0.223 |
| Chemotherapy |
8 (18.2%) |
0 (0%) |
2 (10.5%) |
| Everolimus based therapy |
2 (4.5%) |
3 (11.5%) |
0 (0%) |
| No progression and still on treatment |
27 (61.4%) |
19 (73.1%) |
13 (68.4%) |
| Duration on post discontinuation therapy (months) |
3 (3, 6) |
3 (2, 24) |
23 (4.75, 23) |
0.311 |
| Response according to RECIST criteria after 2nd line treatment (cdk 4/6) |
CR |
12 (27.3%) |
8 (30.8%) |
1 (5.3%) |
0.583 |
| PR |
22 (50%) |
12 (46.2%) |
13 (68.4%) |
| SD |
6 (13.6%) |
4 (15.4%) |
3 (15.8%) |
| PD |
4 (9.1%) |
2 (7.7%) |
2 (10.5%) |
Numerical data are presented as median (IQR) and categorical data are presented as frequency (%), Statistical significance at P value<0.05.
CR: Complete response, PR: Partial response, SD: Stationary disease, PD: Progressive disease coarse, RECIST: Response evaluation criteria in solid
tumors
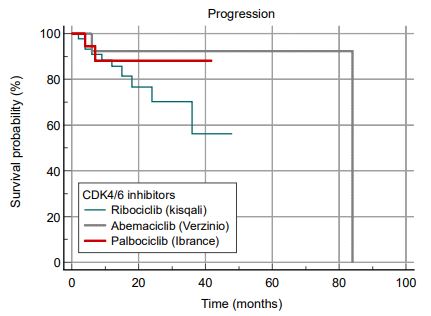
The Kaplan-Meier analysis using the log-rank test revealed that CDK 4/6 inhibitor subtypes had no statistically significant effect on PFS, with progression rates of 22.7%, 11.5%, and 10.5% for Ribociclib, Abemaciclib, and Palbociclib, respectively (Figure 8).
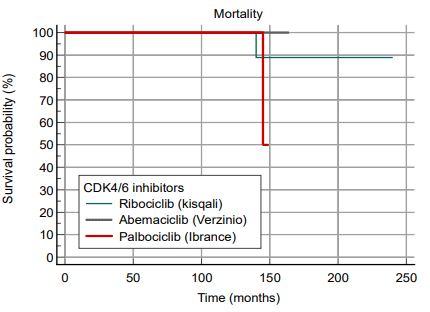
Analysis of the operating system at the date cutoff found no statistically significant difference in mortality rates between CDK 4/6 inhibitor subtypes, with 2.3% getting Ribociclib and 5.3% receiving Palbociclib (Figure 9).
Discussion
Approximately 66% of all breast cancers are hormone-receptor positive, HER2-negative malignant breast neoplasms [2-4]. Adjuvant endocrine treatment can cure the majority of hormone-receptor positive breast tumors in their early stages. However, the number of patients who had recurrence and distant metastases as a result of endocrine therapy resistance is still small.
Three CDK4/6 inhibitors have demonstrated encouraging results in clinical trials: Palbociclib [6-8], Ribociclib [9-12], and Abemaciclib [13,14]. Several clinical studies have shown that combining CDK4/6 inhibitors with endocrine therapy improves Progression-Free Survival (PFS) compared to endocrine treatment alone.
This study’s findings provide supporting evidence that treatment had a statistically significant impact on patients’ PFS, as patients receiving CDK 4/6 inhibitors in combination with endocrine therapy remained free of progression for a longer period of time than those receiving endocrine therapy alone, with an estimated mean of 65.53 months vs. 24.52 months. This pattern of results is consistent with previous study, which found that adding CDK4/6 inhibitors to endocrine treatment significantly improved PFS in persons with hormone receptor-positive, HER2-negative metastatic breast cancer [6,8-11,13].
The current study’s findings confirm the notion that there is no statistically significant difference in overall survival between individuals receiving CDK 4/6 inhibitors in conjunction with endocrine treatment and those getting endocrine therapy alone. These findings support the argument that OS data are only available for PALOMA 1 [7,8], PALOMA 3 [8], and MONALEESA 2 [9].
Two previous meta-analyses [21-23] were insufficient to identify the overall survival advantage, which accounts for the majority of survival. The outcomes of the included RCTs are pending. The US Food and Drug Administration pooled study [24] revealed a non-statistically significant OS benefit across all pooled studies. Because the efficacy data were obtained on April 30, 2018, the overall survival rates for all pooled studies are now incomplete.
Li et al. [25] revealed that CDK4/6 inhibitors improved overall survival (HR 0.79, 95% CI). 0.67–0.93), despite the fact that there were just three randomized controlled trials. Schettini et al. [26] completed a meta-analysis. CDK4/6 inhibitors were proven to improve OS, although they did not include PALOMA-1’s most recent operating system data, which was published in 2017 [7,8]. The latest OS findings from the phase III investigations MONARCH2, MONALEESA 3, and 6 have been revealed [13,14]. A recent meta-analysis extensively examined all six trials, randomized clinical investigations, and updated OS data.
We found that CDK4/6 inhibitors with endocrine therapy significantly improved OS in patients with metastatic luminal breast cancer compared to endocrine therapy alone. We hypothesize that the difference in OS and PFS is attributable to the varied subsequent treatment regimens and the switch from control to CDK4/6 inhibitor therapy. In this example, the increase in PFS was insufficient to justify an OS extension.
The findings clearly suggest that diarrhea, neutropenia, easy fatigability, stomach discomfort, anemia, arthralgia, and muscular weakness occurred in much greater proportions in group A than in group B. Previous studies have shown that adding CDK4/6 inhibitors increased the number of grade 3 and 4 adverse events. The majority of adverse effects impact the blood system, including neutropenia, leucopenia, and anemia. There is a significant difference in the frequency of grade 3 digestive system adverse events, such as diarrhea and vomiting [7,8,21-26].
In our study, CDK 4/6 inhibitors delivered to group A had no statistically significant effect on PFS, with progression rates of 22.7%, 11.5%, and 10.5% for Ribociclib, Abemaciclib, and Palbociclib, respectively. There was no statistically significant difference in OS between the three CDK 4/6 groups, with death rates of 2.3% and 5.3% in patients on Ribociclib and Palbociclib, respectively. This pattern of results is comparable with previous research, which shows that all CDK4/6 inhibitor trials exhibited consistent PFS effects (HRs ranging from 0.50 to 0.59). Meta-analyses revealed no significant differences in PFS across medicines [7,8,22-27].
As a consequence, OS has determined the most essential indicators of pharmacological effectiveness. A network meta-analysis was used to indirectly evaluate the differences in OS and safety profiles across diverse medicines. Their findings reveal that there are no substantial effectiveness differences in OS among the three medications and that effect sizes are clinically important in the majority of cases, independent of statistical significance. However, as expected, there were significant disparities in safety and tolerability [22-27].
Previous studies found significant differences in the safety and tolerability of several CDK4/6 inhibitors. Our study found a strong relationship between the CDK 4/6 subtype and the occurrence of diarrhea, neutropenia, nausea and vomiting, easy fatigability, anemia, renal impairment, and bone pains. Abemaciclib was associated with diarrhea, accounting for 34.6% of cases. Neutropenia is 36.3%, 31.6%, and 11.5% with Ribociclib, Palbociclib, and Abemaciclib, respectively. This conclusion is consistent with recent studies indicating that the most common adverse effects of CDK4/6 inhibitors are hematologic toxicity, which causes a decrease in blood cell counts across many lineages.
Notably, the RORs for Palbociclib and Ribociclib were higher than those for Abemaciclib, and serious systemic infections were uncommon, in line with an earlier study [27]. Hematologic toxicity, the most prominent adverse effect of CDK4/6 inhibitors, is primarily caused by their capacity to inhibit CDK6, a critical regulator of hematopoietic precursor proliferation [28,29]. Palbociclib is similarly effective against both CDK4 and CDK6, but Abemaciclib has a higher affinity for CDK4, resulting in less hematologic damage [28,30].
Furthermore, CDK4/6 inhibitors produce neutropenia primarily through cell cycle suppression rather than chemotherapy-induced DNA damage and consequent death in hematopoietic cells [31].
Study limitations and strengths
Our study has various limitations due to its retrospective nature; a selection bias cannot be totally removed. Another drawback was that our investigation was conducted in a single site with a small number of patients, preventing accurate matching between study groups in terms of comparable staging and hence proper comparison. Furthermore, this study included all patients who came in during this time period, whether they were newly diagnosed or had previously been diagnosed with metastatic luminal breast cancer, resulting in some disparities across study groups.
We suggest more research with a bigger sample size to support or refute our findings. Furthermore, this was the first research to compare the efficacy and safety of three currently available CDK 4/6 inhibitors. Furthermore, this study was carried out in Egypt, where patients and tumors differ from those found in Western nations.
Conclusion
Compared to endocrine therapy alone, CDK4/6 inhibitors significantly improved PFS and OS in patients with hormone receptor-positive, HER2-negative metastatic breast cancer. CDK4/6 inhibitors provided consistent benefits in patients with a variety of patient and tumor characteristics. However, CDK4/6 inhibitors have a higher risk of negative side effects. According to our findings, the kinds of CDK 4/6 inhibitors used showed no statistically significant difference in PFS or OS.
Declarations
Acknowledgements: I’d want to thank everyone who contributed to the work’s creation. This information includes the writers’ opinions, findings, and conclusions.
Authors contributions: SHS and MMA collaborated on the piece’s conception and development. SHS, MMM helped collect data from the filling system. SHS and MMA helped collect, analyze, and interpret the data. SHS and MMA assessed and oversaw the work. SHS and MMA authored the first draft of the text. SHS, MMA perform editing of final draft of the manuscript. All authors contributed to the manuscript editing. All writers agreed on the final version of the manuscript.
Availability of data and materials: Upon reasonable request, the relevant author will provide the data supporting the results of this investigation.
Ethics, approval, and consent to participate: The final protocol was accepted by the research ethics committee of Suez Canal University’s Faculty of Medicine (FOMSCU). Clinical data was obtained with permission from the patients’ filling system.
The confidentiality of the information and patient privacy were taken into account, and no personal information was published.
The data will only be utilized for that specific study; also, patients’ contact information was requested to reduce the chance of erroneous recording and follow-up visits.
Competing interests: The authors stated that they had no competing interests.
Abbreviations: AI: Aromatase Inhibitor; CDK: Cycline-Dependent Kinase; CR: Complete Reaction; ECOG: Eastern Cooperation Oncology Group; ER: Estrogen Receptor; ESMO: European Society for Medical Oncology; ET: Endocrine Treatment; FOMSCU: Faculty of Medicine, Suez Canal University; HER2: Human Epidermal Growth Factor Receptor 2; HR: Hazard Ratio; IQR: Interquartile Range; LHRH: Luteinizing Hormone-Releasing Hormone; MBC: Metastatic Breast Cancer. OS: Overall Survival; PD: Progressive Disease; PFS: Progression-Free Survival; PR: Partial Response; PR Receptor: The Progesterone Receptor; PS: Performance Status; QTc: The Corrected QT Interval; RCT: Randomized Controlled Trials; RECIST: Response Evaluation Criteria in Solid Tumors; ROR: Reporting Odds Ratio; SCUH: Suez Canal University Hospital; SD: Stable Disease; vs.: Versus.
References
- Siegel RL, Miller KD, and Jemal A. Cancer statistics, 2019. CA: A Cancer Journal for Clinicians. 2019; 69: 7-34.
- DeSantis CE, Ma J, Gaudet M, Newman LA, Miller KD, Sauer AG, et al. Breast cancer data for 2019. CA-Cancer J Clin. 2019; 69: 438–51.
- Arpino G, Milano M, and De Placido S. Characteristics of aggressive breast cancer. Breast. 2015; 24: 594–600.
- Perou CM, Sorlie T, Eisen MB, van de Rijn M, Jeffrey S, Rees CA, et al. Molecular images of human breast tumors. Nature. 2000; 406: 747–52.
- Cardoso F, Paluch-Shimon S, Senkus E, Curigliano G, Aapro MS, André F, et al. Fifth ESO-ESMO International Consensus Guidelines for Advanced Breast Cancer (ABC 5). Ann Oncol. 2020; 31: 1623–1649.
- Cristofanilli M, Turner NC, and Bondarenko I. The final analysis of the multicenter PALOMA-3 study compares fulvestrant plus palbociclib to fulvestrant plus placebo for treating hormone-receptor-positive, HER2-negative metastatic breast cancer that has progressed on prior endocrine therapy. Double-blind, phase 3 randomised controlled study. Lancet Oncology. 2016; 17: E270–E7.
- Finn RS, Martin M, Rugo HS, Jones S, Im SA, Gelmon K, et al. Palbociclib plus letrozole in advanced breast cancer. New England Journal of Medicine. 2016; 375: 1925–36.
- Finn RS, Crown JP, Lang I, Boer K, Bondarenko IM, Kulyk SO. A randomized phase 2 research compared palbociclib, a cyclin-dependent kinase 4/6 inhibitor, to letrozole alone as the first-line therapy for oestrogen receptor-positive, HER2-negative, advanced breast cancer. The Lancet Oncology. 2015; 16: 25-35.
- Horobagyi GN, Stemmer SM, Burris HA, Yap YS, Sonke CS, PaluchShimon S, et al. Updated findings from MONALEESA-2, a phase III study comparing first-line ribociclib with letrozole to placebo in hormone receptor-positive, HER2-negative advanced breast cancer patients. Annals of oncology. 2018; 29: 1541-7.
- Slamon DJ, Neven P, Chia S, Fasching PA, De Laurentiis M, Im S-A et al. Ribociclib and Fulvestrant in Hormone-Receptor-Positive, Human Epidermal Growth Factor Receptor 2-Negative Advanced Breast Cancer: A Phase III Randomized Study (MONALEESA-3) (Journal of Clinical Oncology. 2018; 36: 2465).
- Tripathy D, Im S-A, Colleoni M, Franke F, Bardia A, Harbeck N, et al. Ribociclib with endocrine treatment for premenopausal women with hormone-receptor-positive advanced breast cancer (MONALEESA-7): a randomized phase 3 study. Lancet Oncology. 2018; 19: 904–15.
- Horobagyi GN, Stemmer SM, Burris HA, Yap YS, Sonke GS, PaluchShimon S, et al. Ribociclib as a First-Line Treatment for HR-positive, Advanced Breast Cancer. New England Journal of Medicine. 2016; 375: 1738–48.
- Sledge GW, Toi M, Neven P, Sohn J, Inoue K, Pivot X, et al. MO-NARCH 2: Abemaciclib in Combination With Fulvestrant in Women With HR+/HER2-Advanced Breast Cancer Who Have Progressed During Endocrine Therapy. Journal of Clinical Oncology. 2017; 35: 2875.
- Goetz MP, Toi M, Campone M, Sohn J, Paluch-Shimon S, Huober J. MONARCH 3: Abemaciclib as a first treatment for advanced breast cancer. Journal of Clinical Oncology. 2017; 35: 3638.
- Sobhani N, Dell’Angelo A, Pittacolo M, Roviello G, Miccoli A, Corona SP, et al. Updates on CDK4/6 inhibitory strategies and combinations for breast cancer. Cells. 2019; 8: 321.
- Ettl J. Managing adverse events related to cyclin-dependent kinase 4/6 inhibitors. Breast Care. 2019; 14: 86–92.
- George MA, Qureshi S, Omene C, Toppmeyer DL, & Ganesan S. Clinical and pharmacologic differences between CDK4/6 inhibitors in breast cancer. Front Oncol. 2021; 11: 693104.
- Das Majumdar S, Barik S, Pattanaik A, et al. Role of Cyclin-Dependent Kinase 4/6 in Metastatic Breast Cancer: Real-World Data from a Tertiary Care Institute in Eastern India. Cureus. 2024; 16: e52172.
- Wang H, Chow SC. Calculate the sample size for comparing proportions. Wiley Encyclopedia of Clinical Trials. 2007.
- Im SA, Lu YS, Bardia A, Harbeck N, Colleoni M, Franke F, et al. Overall Survival with Ribociclib plus Endocrine Therapy in Breast Cancer. N Engl J Med. 2019; 381: 307-316.
- Turner NC, Slamon DJ, Ro J, Bondarenko I, Im S, Masuda N, et al. Overall Survival with Palbociclib and Fulvestrant in Advanced Breast Cancer. New England Journal of Medicine. 2018; 379: 19261936.
- Deng Y, Ma G, Li W, Wang T, Zhao Y, & Wu Q. CDK4/6 Inhibitors in Combination with Hormone Therapy for HR(+)/HER2(-) Advanced Breast Cancer: A Systematic Review and Meta-analysis of Randomised Controlled Trials. Clin Breast Cancer. 2018; 18: e943–e53.
- Messina C, Cattrini C, Buzzatti G, Cerbone L, Zanardi E, Messina M. A comprehensive review and meta-analysis of randomized trials on CDK4/6 inhibitors for advanced hormone receptor-positive/ HER2-negative breast cancer. Breast Cancer Res Treat. 2018; 172: 9-21.
- Gao JJ, Cheng J, Bloomquist E, Sanchez J, Wedam SB, Singh HS, et al. CDK4/6 inhibitor therapy for patients with hormone receptorpositive, HER2-negative, advanced or metastatic breast cancer: a pooled analysis by the US FDA. The Lancet Oncology. 2020; 21: 250-60.
- Li J, Fu F, Yu L, Huang M, Lin Y, Mei Q, et al. Cyclin-dependent kinase 4 and 6 inhibitors in hormone receptor-positive, human epidermal growth factor receptor-2 negative advanced breast cancer: a meta-analysis of randomized clinical trials.» Breast Cancer research.
- Schettini F, Giudici F, Giuliano M, Cristofanilli M, Arpino G, Del Mastro L. «Overall survival of CDK4/6-inhibitors-based treatments in clinically relevant subgroups of metastatic breast cancer: systematic review and meta-analysis.» J Natl Cancer Inst. 2020.
- Onesti CE; Jerusalem G. «CDK4/6 inhibitors in breast cancer: differences in toxicity profiles and their impact on agent selection.» «A systematic review and meta-analysis.» Expert Rev Anticanc. 2021; 21: 283–98.
- Asghar U, Witkiewicz AK, Turner NC, and Knudsen ES. «The history and future of targeting cyclin-dependent kinases in cancer therapy.» Nat Rev Drug Discov. 2015; 14: 130–46.
- Laurenti E, Frelin C, Xie S, Ferrari R, Dunant C, Zandi S, Neumann A, Plumb I, Doulatov S, Chen J, et al. «CDK6 levels regulate quiescence exit in human hematopoietic stem cells.» Cell Stem Cell. 2015; 16: 302-13.
- Chen P, Lee NV, Hu W, Xu M, Ferre RA, Lam H, et al. «Spectrum and degree of CDK drug interactions predicts clinical performance.» Mol Cancer Ther. 2016; 15: 2273–81.
- Spring LM, Wander SA, Andre F, Moy B, Turner NC, Bardia A. «Cyclin-dependent kinases 4 and 6 inhibitors for hormone receptorpositive breast cancer: past, present, and future.» Lancet. 2020; 395: 817–27.